| Journal of Clinical Gynecology and Obstetrics, ISSN 1927-1271 print, 1927-128X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Gynecol Obstet and Elmer Press Inc |
| Journal website https://jcgo.elmerpub.com |
Original Article
Volume 15, Number 2, June 2026, pages 62-68

Does Office Hysteroscopy Add Value in Polycystic Ovary Syndrome Patients With Normal Transvaginal Ultrasound Findings?
Atef M.M. Darwisha, b, Mohamed M. Fathallaa, Ahmed N. Fetiha, Nermin M. Elsaida, Dina Darwisha, Ahmed A. Abdena
aDepartment of Obstetrics and Gynecology, Faculty of Medicine, Assiut University, Assiut, Egypt
bCorresponding Author: Atef M.M. Darwish, Department of Obstetrics and Gynecology, Faculty of Medicine, Assiut University, Assiut, Egypt
Manuscript submitted February 28, 2026, accepted May 8, 2026, published online June 6, 2026
Short title: Office Hysteroscopy in PCOS
doi: https://doi.org/10.14740/jcgo1662
| Abstract | ▴Top |
Background: This cross-sectional study evaluated the utility of office hysteroscopy in infertile women with polycystic ovary syndrome (PCOS) and normal transvaginal ultrasonography (TVS), compared with unexplained infertility (UI).
Methods: Between December 2021 and December 2024, 150 women were enrolled: 100 with PCOS and 50 with UI. All underwent clinical and hormonal assessment, office hysteroscopy, and endometrial sampling.
Results: In the PCOS group, hysteroscopy identified a thin endometrium (4%), a tiny polyp (1%), and a sub-septate uterus (1%), while a thin endometrium was found in 8% of UI cases. Vascularity abnormalities and Darwish triad micropolyps were observed in both groups. Histopathology revealed chronic endometritis with micropolyps, disordered proliferative endometrium, and occasional hyperplasia, more frequently in PCOS.
Conclusions: No significant clinical correlations were found. Routine hysteroscopy is not recommended in women with normal TVS but may be useful in selected long-standing infertility to detect subtle intrauterine pathology.
Keywords: Polycystic ovary syndrome; Unexplained infertility; Hysteroscopy; Histopathology; Endometrium
| Introduction | ▴Top |
Polycystic ovary syndrome (PCOS) is one of the leading causes of infertility worldwide. While ovulation problems remain central to its pathophysiology, many women continue to experience infertility even after confirming ovulation and ruling out tubal blockage [1]. This highlights the possibility that factors beyond ovulation may contribute to reduced fertility in PCOS. Increasing attention has turned to the role of the endometrium, as some subtle abnormalities in the uterine lining may impair implantation. Similar patterns are also observed in women with unexplained infertility (UI), where standard investigations fail to reveal a cause [2]. Despite many recent studies, the relationship between PCOS and abnormal endometrial function is still not fully understood [3]. Office hysteroscopy (OH), a simple outpatient procedure that allows direct visualization of the uterine cavity, has proven more effective than ultrasound in detecting endometrial abnormalities such as small polyps, fine adhesions, and subtle changes in endometrial morphology [4]. By identifying issues that might otherwise remain hidden, OH provides a valuable tool for refining infertility evaluation. Building on this, the present study used OH to assess the endometrial cavity in infertile women with PCOS and a normal transvaginal ultrasonography (TVS), comparing findings with those from women with UI to explore possible occult endometrial factors. The study highlighted a diagnostic gap common to both groups, rather than comparing their underlying etiologies.
| Materials and Methods | ▴Top |
Study design and setting
This cross-sectional study (ClinicalTrials.gov Identifier: NCT05042895) was conducted at the Infertility Outpatient Clinic and Office Hysteroscopy Unit of Woman’s Health University Hospital, Assiut, Egypt, over a 3-year period between December 2021 and December 2024. The study protocol was reviewed and approved by the Institutional Review Board (IRB: 17200621) of the Faculty of Medicine, Assiut University, Egypt. The work was undertaken in accordance with the provisions of the Declaration of Helsinki.
Study population
A total of 150 infertile women with normal TVS findings were recruited. Infertility was defined as failure to conceive after at least 12 months of regular, unprotected intercourse. Participants were stratified into two groups. Group I (PCOS group) comprised 100 women diagnosed with PCOS according to the Rotterdam criteria (presence of at least two of the following: oligo/anovulation, clinical or biochemical hyperandrogenism, and polycystic ovarian morphology on ultrasound) while group II (UI group) comprised 50 women after standard evaluation (normal semen analysis, confirmed ovulation, tubal patency, and unremarkable TVS).
Sample size calculation
The sample size was estimated with reference to previous studies, such as Amooee et al [5], who investigated 70 women with PCOS and 35 with UI. The calculation was performed using the formula: N = (Δ/Z)2 × P × (100−P), where: Z = 1.96, corresponding to a 95% confidence level, Δ = 12, the acceptable margin of error, and P = 37.5%, the estimated prevalence. Accordingly, the minimum required sample size was 63 women per group, achieving a statistical power of approximately 80% at a 5% significance level. To further strengthen the power and compensate for potential dropouts, the sample size was increased to 100 women in the PCOS group and 50 women in the UI group. The unequal group sizes (n = 100 vs. 50) were intentional, permitting exploratory analyses within the larger PCOS cohort, and followed the design of a previous similar study [5].
Inclusion criteria
The study included women aged 20–38 years with primary or secondary infertility and normal baseline TVS findings. TVS was performed using a high-resolution ultrasound machine (Medison Sonoace X8) with a 7.5 MHz transducer. Endometrial thickness, echogenicity, and uterine morphology were assessed. In patients with PCOS, ovarian volume and antral follicle count were also recorded. Only women with normal endometrial thickness and pattern, absence of intracavitary pathology, and normal uterine morphology were included.
Exclusion criteria
Exclusion criteria were abnormal TVS findings suggestive of intrauterine pathology, such as thickened endometrium in the proliferative phase, features of endometrial hyperplasia, endometrial polyps, Mullerian anomalies, suspected intrauterine adhesions, or fibroids distorting the cavity. Patients with a history of intrauterine surgery within the previous 6 months (e.g., dilation and curettage or hysteroscopy) were also excluded. Additional exclusion criteria included known systemic diseases affecting fertility (e.g., uncontrolled diabetes, thyroid disorders, hyperprolactinemia) and refusal to participate.
Comprehensive diagnostic evaluation
At the infertility outpatient clinic, all participants underwent detailed history taking, including duration and type of infertility, menstrual pattern, obstetric history, and previous treatments. General and gynecological examinations were performed, with particular attention to body mass index (BMI) and clinical signs of hyperandrogenism (hirsutism, acne, androgenic alopecia).
In the outpatient laboratory, baseline hormonal profiling was conducted during the early follicular phase (postmenstrual days 2–4). Blood samples were analyzed for follicle-stimulating hormone (FSH), luteinizing hormone (LH), estradiol (E2), anti-Mullerian hormone (AMH), thyroid-stimulating hormone (TSH), and prolactin using enzyme-linked immunosorbent assay (ELISA).
All participants with normal TVS findings subsequently underwent OH in the early proliferative phase (cycle days 6–10) using a vaginoscopic, anesthesia-free approach as previously described by our team [6]. A 2.9-mm, 30° rigid hysteroscope (Karl Storz, Tuttlingen, Germany) with continuous saline flow was utilized without cervical dilation. The cervical canal and internal os were inspected, followed by systematic evaluation of the endometrial cavity for endometrial texture, vascularity, cavity shape, and focal lesions (polyps, fibroids, adhesions, or congenital anomalies). Special attention was given to the Darwish triad [7], tubal ostium, converging walls, and the cone-shaped proximal part of the fallopian tubes with its characteristic black spot, by rotating the telescope toward both cornual regions. At the end of OH, 10–30 mL methylene blue dye was injected through the side channel of OH, and the hysteroscopist waited a few minutes to allow staining of the endometrium. Healthy endometrium does not stain while pathologic cells stain blue (Fig. 1). This “chromohysteroscopy” aims to localize any abnormal endometrial area to guide biopsy taking as previously described [8]. Abnormal findings, when present, were documented using digital imaging. Endometrial thickness was assessed by advancing the telescope to the uterine fundus and then gently withdrawing it along the posterior wall toward the cervix. A deep furrow along the pathway was considered suggestive of thickened endometrium, the absence of a furrow indicated a thin endometrium, while a shallow furrow was regarded as normal. At the end of hysteroscopic evaluation, adequate endometrial sample was taken primarily from any methylene blue-stained areas. In cases with a normal chromohysteroscopic appearance, a systematic sampling was performed from the mid-fundal, anterior, and posterior walls using a 4-mm Novak curette. All samples were sent for histopathological assessment. A positive hysteroscopic finding was defined as any visible abnormality (e.g., polyp, adhesion, focal congestion, micropolyp). Histopathology was considered the reference standard.
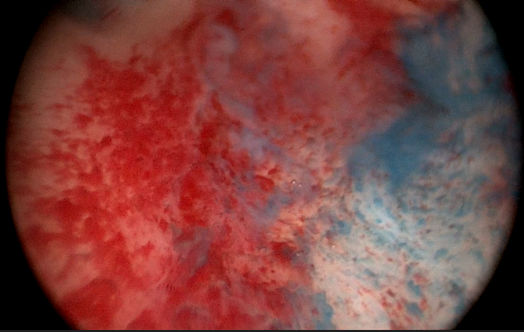 Click for large image | Figure 1. Chromohysteroscopy: Methylene blue staining of pathologic endometrium. |
Before discharge, patients were asked to rate their satisfaction with the “one-stop” approach combining clinical assessment, hormonal testing, OH, and endometrial sampling in a single visit. Analgesics were prescribed on an as-needed basis. Patients were subsequently contacted by the junior investigator (NE) to discuss histopathology and laboratory results, as well as to define the further management plan.
Study outcomes
The primary outcome was the prevalence of abnormal hysteroscopic findings in PCOS patients with normal TVS. Secondary outcomes were: 1) the prevalence of abnormal histopathology as the gold standard diagnostic tool; and 2) a comparison of findings between the PCOS group and a UI group.
Data collection and statistical analysis
Data were analyzed using SPSS software, version 22.0 (IBM Corp., Armonk, NY, USA). Normality of continuous variables was assessed with the Shapiro–Wilk test. Normally distributed variables were summarized as mean ± standard deviation (SD), whereas skewed variables were expressed as median with interquartile range (IQR). Comparisons between the PCOS and UI groups were performed using the independent-samples t-test for normally distributed data and the Mann–Whitney U test for non-normally distributed data. Categorical variables were reported as frequencies and percentages and compared using the Chi-square test or Fisher’s exact test where appropriate (expected cell count < 5). Correlation analyses were conducted using Pearson’s correlation for normally distributed variables and Spearman’s correlation for non-normally distributed variables. A P value < 0.05 was considered statistically significant.
| Results | ▴Top |
The study included infertile women with a normal endometrial appearance on TVS, who were classified into two groups. Group A comprised 100 women with PCOS-related infertility, while group B included 50 women with UI. Both groups were comparable in terms of sociodemographic and clinical characteristics, except for significantly higher weight and BMI observed in group A (Table 1). The hormonal profiles of both groups are presented in Table 2, which shows a significantly higher LH level in group A. Despite the normal endometrial pattern on TVS, endometrial thickness was significantly greater in group A (8.86 ± 1.64 mm) compared to group B (6.06 ± 1.61 mm, P < 0.01). As shown in Table 3, there was no statistically significant difference in hysteroscopic findings between the two groups. Micropolyps were seen inside Darwish triad in six (6%) and four (8%) cases in both groups, respectively (Fig. 2). Congested endometrial patches were seen in four (4%) and one (2%) cases in both groups, respectively, while micropolyps were seen in one case (1%) in PCOS group (Fig. 3). Methylene blue staining at the end of OH was done in all cases to localize pathologic areas (Fig. 1). Additionally, there was no significant association between hysteroscopic endometrial patterns and clinical or hormonal parameters in either group, except for a higher FSH level observed in women with abnormal hysteroscopic patterns within group A. Histopathological findings for both groups are summarized in Table 4. No cases of hyperplasia with atypia or malignancy were reported in either group. Table 5 presents the diagnostic indices of hysteroscopy for detecting abnormal endometrial pathology. Hysteroscopy demonstrated high sensitivity, specificity, and positive predictive value, but a notably low negative predictive value when compared with histopathological diagnosis.
 Click to view | Table 1. Demographic Data in Both Groups |
Click to view | Table 2. Hormonal Profile in Study Groups |
Click to view | Table 3. Hysteroscopic Findings in Study Groups |
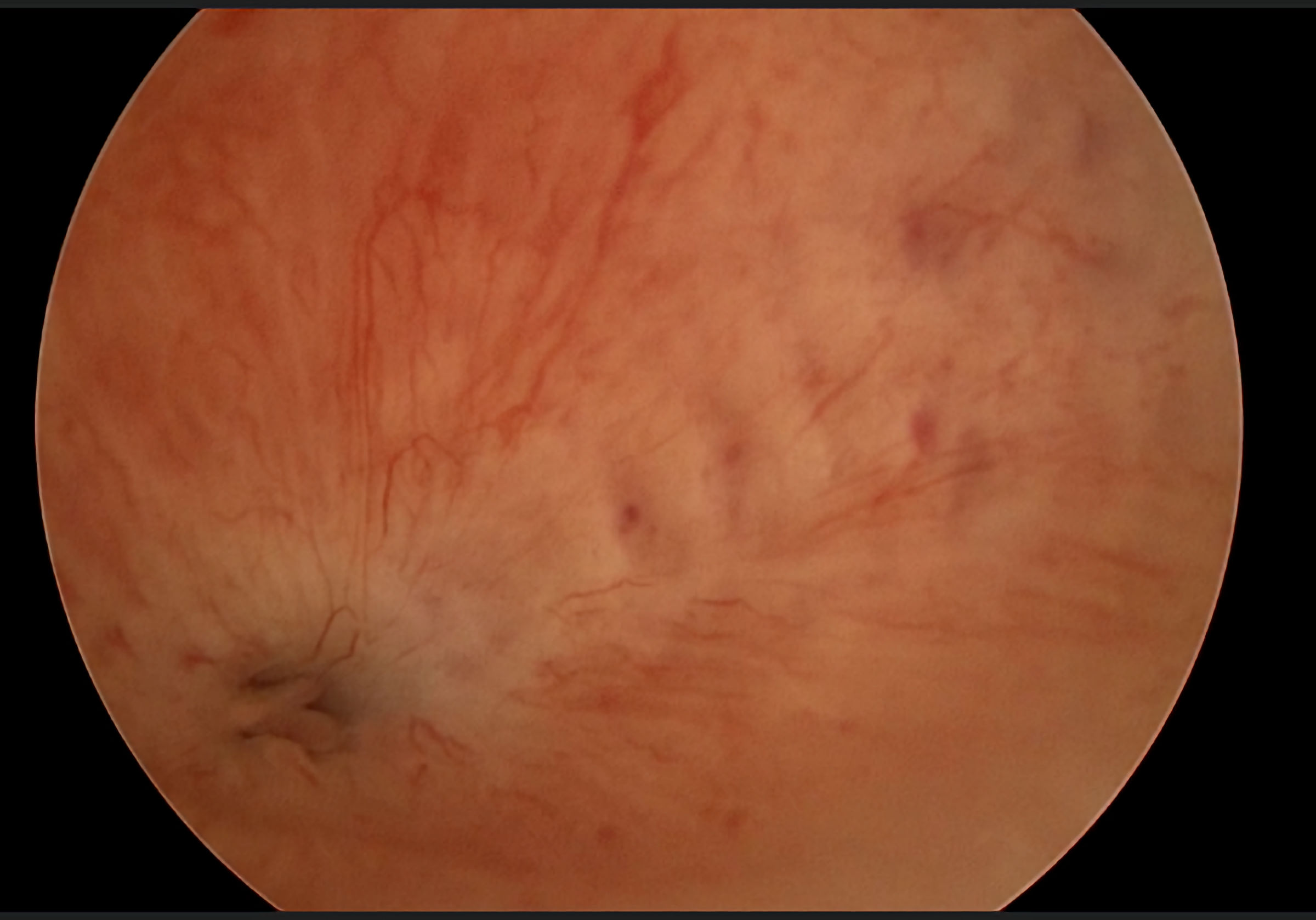 Click for large image | Figure 2. Hysteroscopic appearance of micropolyps at Darwish triad. |
 Click for large image | Figure 3. Hysteroscopic appearance of congested endometrium and micropolyps. |
Click to view | Table 4. Histopathologic Findings in Both Groups |
Click to view | Table 5. Diagnostic Indices of Office Hysteroscopy Versus Histopathology in Both Groups |
| Discussion | ▴Top |
In women with PCOS, the endometrium is often disrupted due to chronic anovulation, prolonged unopposed estrogen exposure, progesterone resistance, and insulin resistance. These mechanisms contribute to an increased risk of endometrial thickening, hyperplasia, and, over time, even endometrial carcinoma following years of unopposed estrogen stimulation [3]. One study reported significantly greater endometrial thickness in the PCOS group (11.1 mm) and in women with insulin resistance (9.6 mm), compared with controls (6.2 mm; P < 0.001) [9].
TVS is now widely available in most gynecology clinics and plays a crucial role in the diagnostic workup of PCOS. Among women with PCOS, especially those with oligomenorrhea or irregular cycles, the risk of endometrial hyperplasia is higher than in women with regular cycles. In the present study, the wide availability of TVS was a key reason for selecting only cases with normal TVS findings, as most abnormal endometrial pathologies can be reliably detected during routine scanning.
OH, on the other hand, has been increasingly adopted in the evaluation of various gynecological conditions with excellent outcomes. At our institution, the OH unit was established over 35 years ago and has been extensively applied in cases of infertility [6], abnormal uterine bleeding [10], and Mullerian duct anomalies [11]. OH allows accurate diagnosis of intrauterine abnormalities, such as endometrial polyps, while also providing the opportunity for targeted endometrial or even myometrial biopsy in a minimally invasive and well-tolerated manner.
In this study, thin endometrium was detected hysteroscopically in four cases from each group, which is uncommon in PCOS. This finding may be explained by hyperandrogenism, which inhibits endometrial growth and differentiation and impairs decidualization during the luteal phase [12]. The clinical significance of thin endometrium in PCOS has been highlighted in several studies. For example, reduced endometrial thickness (≤ 8 mm) was independently associated with an increased risk of preterm birth (PTB), low birthweight (LBW), and small-for-gestational-age (SGA) infants in women with PCOS [13]. However, thin endometrium is more reliably measured by TVS, whereas the hysteroscopic thickness assessment used in this study is subjective and lacks precise measurement.
The relatively low prevalence of abnormal hysteroscopic endometrial findings in this study (6% and 4% in groups A and B, respectively) can be attributed to the strict inclusion criteria, which excluded any suspected endometrial pathology. This contrasts with other reports that described higher prevalence rates of 32% [14] and 24% [15]. A strength of hysteroscopy, however, lies in its ability to detect chronic endometritis (CE). In this study, CE was hysteroscopically suspected in 5% of PCOS cases and 2% of UI cases, mainly in the form of micropolyps and congested endometrium. Various hysteroscopic patterns of CE have been described, including hemorrhagic spots, stromal edema, endometrial micropolyps ≤ 1 mm, hyperemic areas with central white points, hypervascularity, and filmy adhesions [16]. In our study, endometrial congestion was the most common diagnostic clue, consistent with previous reports [17]. When compared to histopathology as the reference standard, hysteroscopy showed a notably low negative predictive value, indicating that a normal hysteroscopic appearance does not reliably rule out histologic abnormalities, such as CE or disordered proliferation.
Histopathology confirmed CE in 14% of PCOS cases and 8% of UI cases, despite relying only on hematoxylin and eosin (H&E) staining. The diagnostic accuracy of H&E is limited, as plasma cells can be difficult to differentiate from leukocytes in the stroma. Immunohistochemistry for syndecan-1 (CD138), which specifically identifies plasma cells, offers higher accuracy, as positive cells appear brown with CD138 staining. The relatively high prevalence of CE in our series, despite the limitations of H&E, supports the recommendation to include CE evaluation and endometrial sampling in infertile women with PCOS or UI [18].
In addition, two cases of focal simple endometrial hyperplasia were identified in the PCOS group, despite normal TVS and even normal hysteroscopic appearance. These false negatives highlight the importance of endometrial sampling as the diagnostic gold standard, especially in women presenting with menstrual irregularities or suspected poor endometrial receptivity. Distorted proliferative endometrium was also observed in eight PCOS patients, suggesting abnormal endometrial growth secondary to persistent unopposed estrogen stimulation. This finding represents a potential risk factor for endometrial hyperplasia and, in some cases, endometrial carcinoma [19], and therefore warrants careful interpretation.
Finally, OH was also utilized to investigate potential anatomic tubal factors in both groups. As previously reported [17], OH provides valuable assessment of the proximal fallopian tubes, offering not only anatomic but also functional information, such as tubal patency and peristalsis [20]. In this study, intratubal micropolyps occluding the distal tube were identified in six PCOS cases and four UI cases and were successfully excised using flexible micro-grasping forceps, thereby potentially restoring sperm and embryo passage. Further studies are needed to evaluate the reproductive impact of such interventions.
This study has several limitations that should be considered when interpreting the results. First, the cross-sectional design carries an inherent risk of selection bias. The study population may not be fully representative of all women with PCOS, as only those without sonographic abnormalities were included. This selection may have led to an underestimation of the true prevalence of hysteroscopic and histopathological abnormalities. Second, caution is warranted in interpreting correlations between clinical or hormonal parameters and endometrial pathologies, given that the sample does not reflect the broader PCOS population. Moreover, the effect of treating hysteroscopic or histopathological abnormalities on conception rates and pregnancy outcomes remains uncertain and requires further investigation. An important limitation of this study is the lack of CD138 testing, as the diagnosis of CE relied solely on H&E staining. Given the low sensitivity of H&E for detecting plasma cells, histopathology likely underestimated the true prevalence of CE. Consequently, the “gold standard” used for accuracy calculations (Table 5) is itself imperfect, which probably inflates the estimated sensitivity and specificity of hysteroscopy for CE. Additionally, the low prevalence of abnormalities (6% in group A) is almost certainly an underestimation, particularly for CE. Finally, additional studies are needed to identify the subgroup of women with PCOS who are most likely to benefit from hysteroscopic evaluation.
Conclusions
Routine OH is not recommended for women with PCOS or UI who demonstrate normal findings on TVS, as it primarily detects minor endometrial changes while adding unnecessary cost, stress, and invasiveness to the infertility workup. Nonetheless, OH may have a role in carefully selected cases of long-standing infertility, after exclusion of other contributing factors, to identify subtle intrauterine abnormalities such as CE, small morphological lesions, or Darwish triad micropolyps.
Acknowledgments
The authors thank the patients for consenting to participate in this study.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
Written informed consent was obtained from all participants before enrolment.
Author Contributions
AD conceptualized and designed the study, interpreted the data, wrote the discussion, and revised the full manuscript. MF supervised the study and critically reviewed the manuscript. AF supervised the study and critically reviewed the manuscript. NE conducted the study, recruited participants, collected data, performed statistical analysis, and drafted the manuscript. DD and AA substantively revised the manuscript.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
| References | ▴Top |
- Teede HJ, Tay CT, Laven J, Dokras A, Moran LJ, Piltonen TT, Costello MF, et al. Recommendations from the 2023 International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. Fertil Steril. 2023;120(4):767-793.
doi pubmed - Zegers-Hochschild F, Crosby JA, Musri C, Petermann-Rocha F, Borges de Souza MDC, Martinez AG, Azambuja R, et al. ART in Latin America: the Latin American Registry, 2020. Reprod Biomed Online. 2023;47(2):103195.
doi pubmed - Xue Z, Li J, Feng J, Han H, Zhao J, Zhang J, Han Y, et al. Research progress on the mechanism between polycystic ovary syndrome and abnormal endometrium. Front Physiol. 2021;12:788772.
doi pubmed - Yao Y, Lv W, Xie X, Cheng X. The value of hysteroscopy and transvaginal ultrasonography in the diagnosis of endometrial hyperplasia: a systematic review and meta-analysis. Transl Cancer Res. 2019;8(4):1179-1187.
doi pubmed - Amooee S, Akbarzadeh-Jahromi M, Motavas M, Zarei F. Comparing endometrial hysteroscopic and histological findings of infertile women with polycystic ovary syndrome and unexplained infertility: A cross-sectional study. Int J Reprod Biomed. 2019;18(1):33-40.
doi pubmed - Darwish AM, Hassanin AI, Abdel Aleem MA, Mohammad II, Aboushama IH. Routine vaginoscopic office hysteroscopy in modern infertility work-up: a randomized controlled trial. Gynecological Surgery. 2014;11:185-189
- Darwish AM. Darwish Hysteroscopic Triad: A Missed Anatomic Landmark. Journal of Gynecologic Surgery. 2021;37(1):94-95.
doi - Darwish AMM, Darwish DAM. A chromo-hysteroscopic documentation of a transverse fundal endometrial defect. Arch Gynecol Obstet. 2024;309(4):1697-1698.
doi pubmed - Iatrakis G, Tsionis C, Adonakis G, Stoikidou M, Anthouli-Anagnostopoulou F, Parava M, Vouxinou A, et al. Polycystic ovarian syndrome, insulin resistance and thickness of the endometrium. Eur J Obstet Gynecol Reprod Biol. 2006;127(2):218-221.
doi pubmed - Darwish AM, Sayed EH, Mohammad SA, Mohammad II, Hassan HI. Reliability of out-patient hysteroscopy in one-stop clinic for abnormal uterine bleeding. Gynecologic Surgery. 2012;9(3):289-295.
- Darwish AM, Khalaf M, Ahmed GM. Reliability of office hysteroscopic reconstructive surgery (HRS) in a tertiary-hospital performing conventional day-case HRS for 30 years. Journal of Gynecologic Surgery. 2022;38(1):57-65.
doi - Sanchez-Garrido MA, Tena-Sempere M. Metabolic dysfunction in polycystic ovary syndrome: Pathogenic role of androgen excess and potential therapeutic strategies. Mol Metab. 2020;35:100937.
doi pubmed - Huang J, Lin J, Xia L, Tian L, Xu D, Liu P, Zhu J, et al. Decreased Endometrial Thickness Is Associated With Higher Risk of Neonatal Complications in Women With Polycystic Ovary Syndrome. Front Endocrinol (Lausanne). 2021;12:766601.
doi pubmed - Ibrahim MA, Abd Elsamie AA, Bakry MS, Abou-Beih SS. Correlation between hysteroscopy finding and chronic endometritis in unexplained primary infertility. FUMJ. 2022;10(3):40-50.
doi - Kitaya K, Yasuo T, Yamaguchi T, Morita Y, Hamazaki A, Murayama S, Mihara T, et al. Construction of deep learning-based convolutional neural network model for automatic detection of fluid hysteroscopic endometrial micropolyps in infertile women with chronic endometritis. Eur J Obstet Gynecol Reprod Biol. 2024;297:249-253.
doi pubmed - Bouet PE, El Hachem H, Monceau E, Gariepy G, Kadoch IJ, Sylvestre C. Chronic endometritis in women with recurrent pregnancy loss and recurrent implantation failure: prevalence and role of office hysteroscopy and immunohistochemistry in diagnosis. Fertil Steril. 2016;105(1):106-110.
doi pubmed - Furui M, Ito A, Fukuda Y, Sekiguchi M, Nakaoka K, Hayashi Y, Tamaki Y, et al. Endometrial congestion is the only hysteroscopic finding indicative of chronic endometritis. PLoS One. 2024;19(6):e0303041.
doi pubmed - Zargar M, Ghafourian M, Nikbakht R, Mir Hosseini V, Moradi Choghakabodi P. Evaluating chronic endometritis in women with recurrent implantation failure and recurrent pregnancy loss by hysteroscopy and immunohistochemistry. J Minim Invasive Gynecol. 2020;27(1):116-121.
doi pubmed - Mangla M, Palo S, Kanikaram PK, Raja Shekar P, Setty A. Comparative immuno-profiling of proliferative and disordered proliferative endometrium in anovulatory abnormal uterine bleeding. J Obstet Gynaecol Res. 2025;51(8):e70032.
doi pubmed - Darwish AM, Darwish DA. Hysteroscopic darwishscope test versus bubble flow patency test for normal and hydrosalpingeal fallopian tubes. Journal of Gynecologic Surgery. 2022;38(1):49-56.
doi
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Clinical Gynecology and Obstetrics is published by Elmer Press Inc.