| Journal of Clinical Gynecology and Obstetrics, ISSN 1927-1271 print, 1927-128X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Gynecol Obstet and Elmer Press Inc |
| Journal website https://jcgo.elmerpub.com |
Case Report
Volume 15, Number 2, June 2026, pages 73-78

A Case of Normal Uterus With Bicollis and Vaginal Septum: A Challenge to the Classical Theory of Mullerian Duct Fusion
Lewis Nancarrowa, c, d, Beth Hankinsonb, Marwa Fakhreldina, c
aHewitt Fertility Centre, Liverpool Women’s Hospital, NHS Foundation Trust, Member of Liverpool Health Partners, Liverpool, UK
bDepartment of Radiology, Royal Liverpool Hospital, Member of Liverpool Health Partners, Liverpool, UK
cCentre for Women’s Health Research, Department of Women’s and Children’s Health, Institute of Life Course and Medical Sciences, Faculty of Health and Life Sciences, University of Liverpool, Liverpool, UK
dCorresponding Author: Lewis Nancarrow, Hewitt Fertility Centre, Liverpool Women’s Hospital, NHS Foundation Trust, Member of Liverpool Health Partners, Liverpool L8 7SS, UK
Manuscript submitted January 2, 2026, accepted March 9, 2026, published online June 6, 2026
Short title: Normal Uterus With Bicollis and Vaginal Septum
doi: https://doi.org/10.14740/jcgo1629
| Abstract | ▴Top |
Mullerian duct abnormalities (MDAs) are common, known to occur in 5% of women and can be categorized using a number of different classification systems, including those from the American Society for Reproductive Medicine (ASRM) or the European Society of Human Reproduction and Embryology (ESHRE). The most popular developmental theories assume that Mullerian duct fusion begins caudally then extends cranially. However, these theories cannot explain isolated cervical or vaginal MDA. Our case of a 20-year-old with isolated cervical duplication and longitudinal vaginal septum but normal uterus, diagnosed at the time of hysteroscopy, calls into question this hypothesis, instead supporting the theory of segmental or bidirectional fusion of the Mullerian ducts.
Keywords: Mullerian duct abnormality; Vaginal septum; Hysteroscopy; Embryology
| Introduction | ▴Top |
Mullerian duct abnormalities (MDA) can occur in 5.5–6.7% of the general population [1, 2]; however, the prevalence increases to 7.3–8% in infertile women, 13.3–16.7% in women with recurrent miscarriage and up to 24.5% in those patients who are infertile and have recurrent miscarriages [1, 2]. However, the prevalence of isolated cervical duplication and/or longitudinal vaginal septum is extremely rare and has been reported in only a few case reports previously [3]. The historical theory of embryological development of the female genital system is assumed to occur with elongating of the Mullerian ducts, which attach and fuse to the urogenital sinus [4]. The fusion begins caudally extending cranially, followed by rearrangement of the epithelial cells and subsequent absorption of the septum [4–6] (Fig. 1).
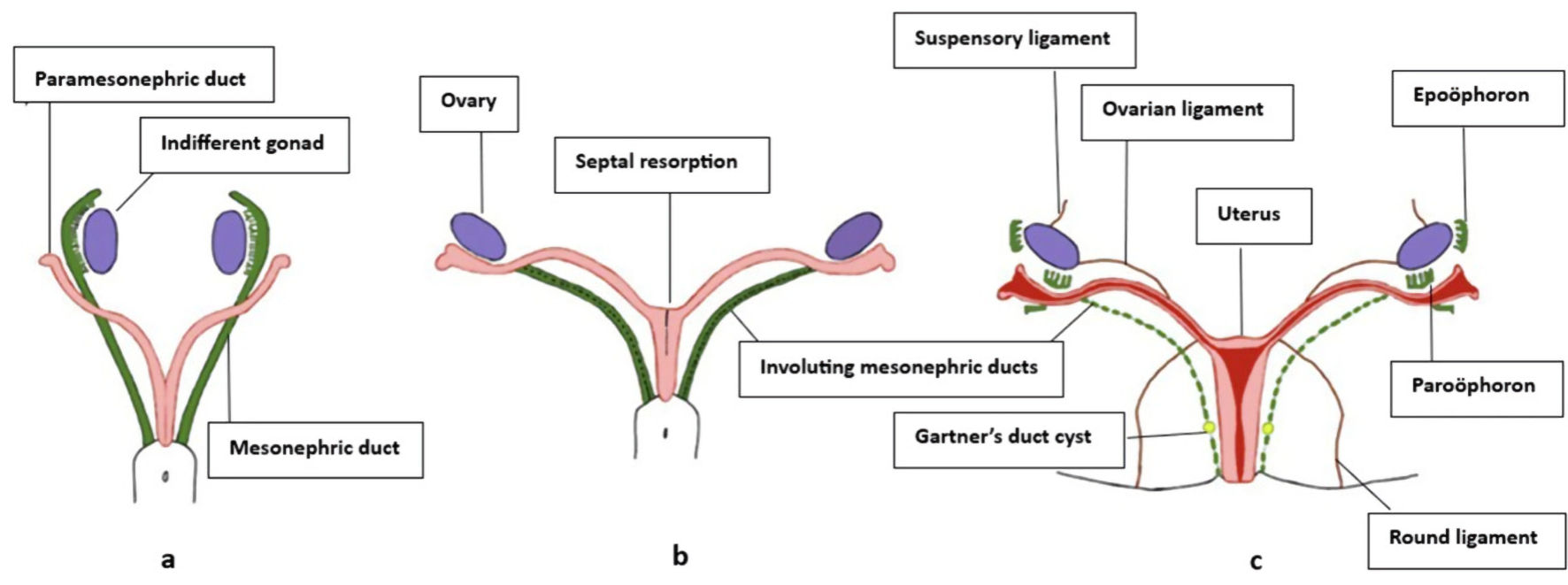 Click for large image | Figure 1. Development of female internal genitalia. (a) Undifferentiated gonads are present with Mullerian ducts lateral to mesonephric ducts cranially and medial caudally. (b) In females, mesonephric ducts regress as Mullerian ducts fuse and the septum is resorbed. (c) Uterus, cervix, and upper vagina, with mesonephric remnants such as the epoophoron, paroophoron, and Gartner’s duct cysts [5]. |
Both the American Society of Reproductive Medicine (ASRM) [7] and European Society of Human Reproduction and Embryology (ESHRE) [8] have produced classification systems for MDAs, which encompass a wide spectrum of this variable condition. Common MDAs include bicornuate uterus, uterus didelphys, septate uterus, unicornuate uterus and vaginal septum. We present a rare case of a bicollis uterus with an upper vaginal septum, confirmed during hysteroscopy and supported by a review of similar case reports. This finding challenges the widely accepted theory of caudal-to-cranial Mullerian duct fusion, instead suggesting alternative mechanisms—such as bidirectional or segmental fusion—that may better explain isolated cervical anomalies, as in our case.
| Case Report | ▴Top |
A 20-year-old patient was referred to the secondary care unit with post-coital bleeding and dyspareunia. She also found insertion of tampons uncomfortable, and when she examined herself, she felt a fleshy lump in the anterior vaginal wall. She had been on the combined oral contraceptive pill for irregular, painful periods. She had never been pregnant and was not trying to conceive, although she was in a relationship. She had a past medical history of recurrent urinary tract infections and cystitis as a child, but this did not continue into adulthood, and she has no current medical conditions.
On examination, she had normal external genitalia. However, there was a vertical midline vaginal septum extending through the upper two-thirds of the vagina. Additionally, there was a duplication of the cervix, with the two cervices positioned on either side of the vaginal septum in a right-to-left arrangement.
The ultrasound report queried whether there was a uterus didelphys, as two clear cervices were noted on transverse view (Fig. 2); however, there was no three-dimensional (3D) probe at the time to determine the true nature of the cavity.
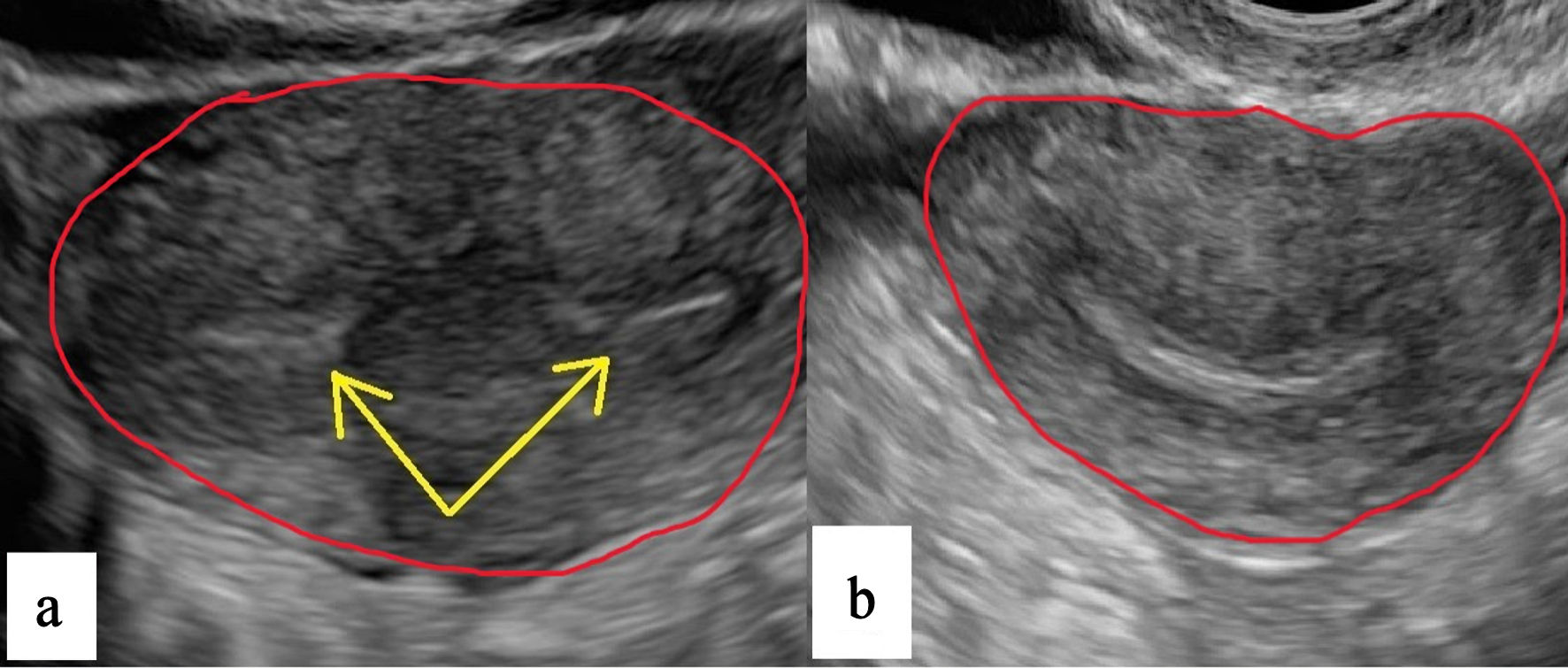 Click for large image | Figure 2. Transvaginal ultrasound. (a) View of two cervices (yellow arrows). (b) Transverse view of normal uterus. |
The patient was sent for a magnetic resonance imaging (MRI) scan, which found an unremarkable uterus (Fig. 3) with normal fundal contour and no associated Mullerian abnormality.
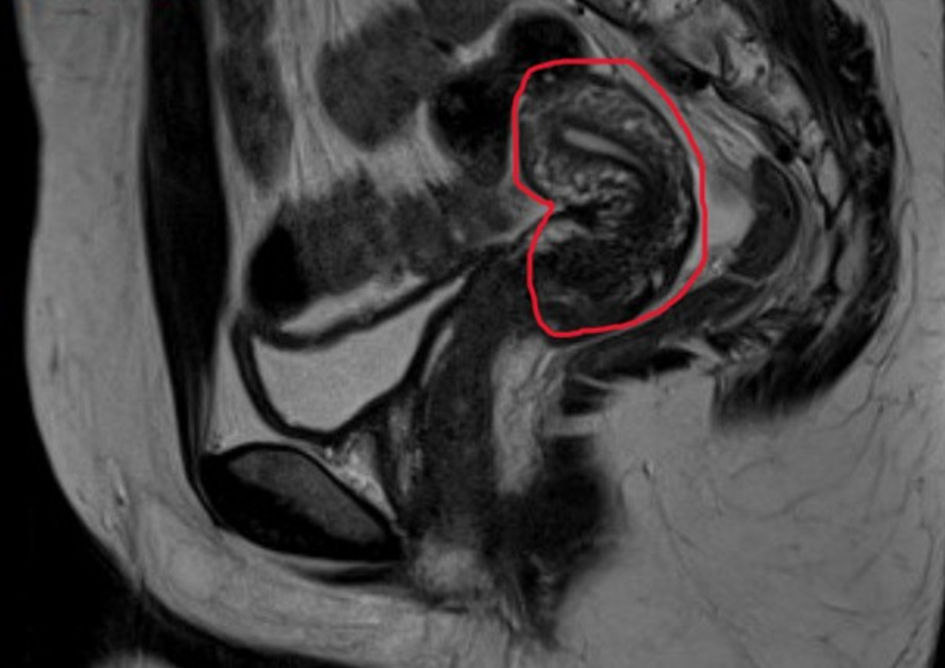 Click for large image | Figure 3. MRI of normal sagittal view of uterus. MRI: magnetic resonance imaging. |
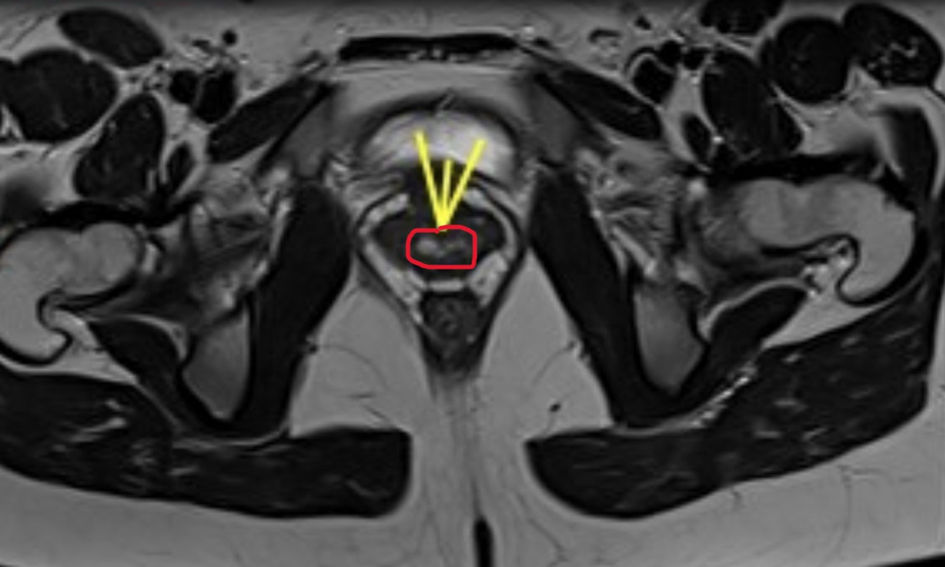
It was noted that there was a single cervix, which duplicated at the level of the external os but fused prior to the uterine cavity. It was also suggested that the duplication may involve the inferior aspect of the cervix, and a septum extends through the upper two-thirds of the vagina (Figs. 4–6). There were no renal abnormalities detected on the MRI scan.
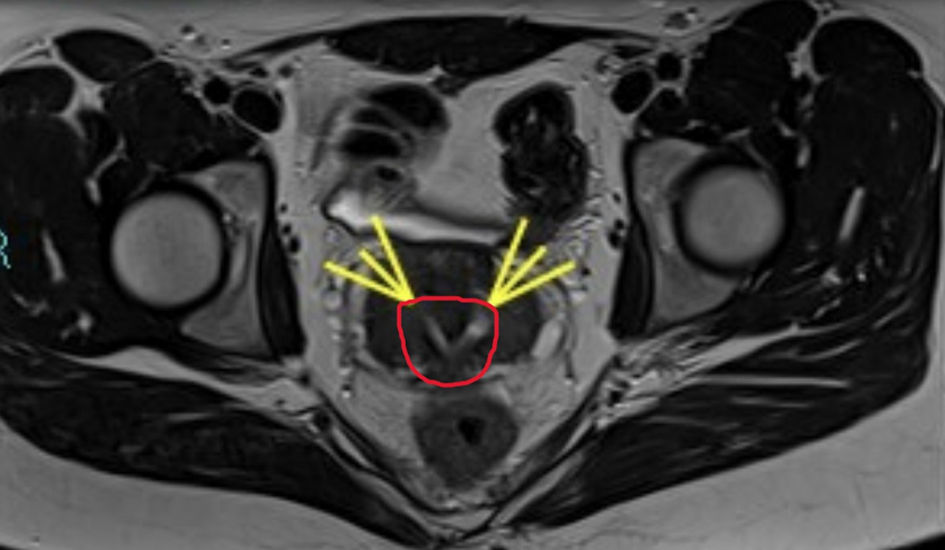 Click for large image | Figure 4. MRI of double cervix at external os (yellow arrows). MRI: magnetic resonance imaging. |
 Click for large image | Figure 5. MRI of vaginal septum (yellow arrows). MRI: magnetic resonance imaging. |
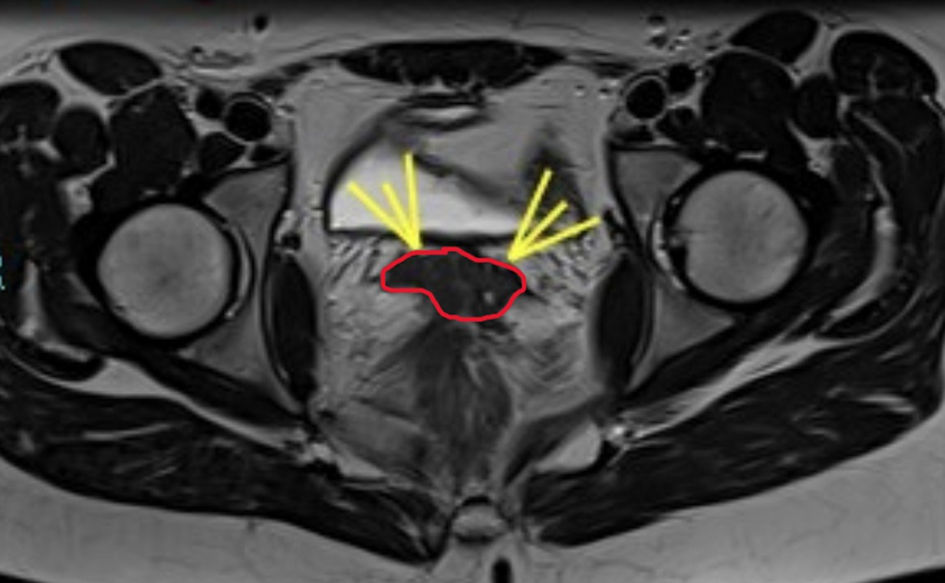 Click for large image | Figure 6. MRI showing duplication of vagina (yellow arrows). MRI: magnetic resonance imaging. |
The patient was subsequently booked for a hysteroscopy and resection of the vaginal septum. The septum did extend from the external os to the lower third of the vagina, although it did not seem to extend into the cervix. The two distinct cervices (right and left side) seemed to be fused medially as evident in the MRI images. The septum was resected without complication. Hysteroscopy was performed through both cervices, where it was then clear that both cervices communicated with the one normal uterine cavity. The patient made an unremarkable recovery and was followed up 4 months after surgery, where she noticed an improvement in her dyspareunia and was subsequently discharged.
| Discussion | ▴Top |
The embryologic sequence to the formation of the female genital tract is most commonly based on the theory from Crosby and Hill back in the 1960s [9]. This theory suggests that Mullerian duct fusion occurs between the 11th and 13th week of gestation, with fusion of the ducts from a caudal to cranial fashion and subsequent absorption of the septum between the two ducts [9]. Based on current MDA classifications from both ESHRE and ASRM, they would seem to concur with this caudal to cranial fusion hypothesis [7, 8].
However, subsequent embryologic investigations have demonstrated that development of the distal genital tract is more complex than a strictly linear fusion process [10]. Vaginal formation involves coordinated interaction between the Mullerian ducts and the urogenital sinus, with significant contribution from the Mullerian tubercle and sinovaginal bulbs [10]. These findings have supported alternative mechanistic interpretations of MDAs, particularly those affecting the cervix and vagina.
Previous concepts of Mullerian duct fusion may initiate at the uterine isthmus, with subsequent cranial and caudal progression [3, 11]. This theory aligns more coherently with our case and other rare reports, where cervical duplication occurs without uterine anomaly [3, 12–15]. The presence of a single uterine corpus with duplicated cervices is consistent with a localized disturbance of caudal fusion or resorption rather than a global duct fusion defect. The bidirectional theory therefore offers a mechanistic explanation for how cervical duplication may occur independently of uterine duplication.
The Embryological–Clinical Classification (ECC) of Female Genital Malformations provides a developmentally structured system that links anomalies to specific embryologic components. Within this framework, our case is most appropriately categorized as a Mullerian tubercle anomaly, specifically 3B.2.1—double cervix with septate vagina [10].
This classification localizes the anomaly to the distal cervicovaginal interface and emphasizes disruption of fusion or resorption at the level of the Mullerian tubercle rather than primary failure of uterine duct fusion.
ASRM and ESHRE classifications remain the most widely used systems in clinical practice. Both provide structured, morphology-based frameworks that are relatively straightforward to interpret and apply in routine diagnostic and surgical settings. Their strength lies in their practical usability, reproducibility, and familiarity among clinicians.
The ASRM system is intuitive and broadly adopted, but it has limited granularity in isolated cervical or complex cervicovaginal anomalies. The ESHRE system permits independent categorization of uterine, cervical, and vaginal components (e.g., U0C2V1) (Fig. 7) [8], allowing more detailed morphological description.
 Click for large image | Figure 7. Diagram of genital tract of patient (U0, C2, V1 using ESHRE classification). ESHRE: the European Society of Human Reproduction and Embryology. |
In contrast, the ECC is explicitly grounded in embryologic origin. While it may be less immediately familiar and somewhat more conceptually demanding to apply, it offers greater developmental precision and is more concise in defining the specific embryologic variance responsible for a given MDA. In cases such as ours—where the anomaly is distal and does not conform neatly to uterine fusion categories—the ECC provides a clearer etiologic localization.
Importantly, these systems should not be viewed as competing but rather as complementary. ASRM and ESHRE offer accessible and clinically practical categorization, whereas the ECC provides enhanced embryologic resolution. In our case, the bidirectional fusion theory provides a mechanistic explanation, and the ECC supplies a structurally precise classification, together offering a coherent developmental interpretation.
A literature search reveals only a handful of similar cases. Deo et al (2008) reported a bicollis uterus with vaginal septum following cervical smear [12]. She had resection of septum and then went on to conceive naturally and have a spontaneous vaginal delivery with a third-degree tear. Similarly, at routine checkup, Morales-Rosello et al (2011) described a bicervical (anteroposterior disposition in contrast to our lateral disposition) uterus with a single corpus and normal vagina [14]. This patient had one uncomplicated vaginal delivery and no other pregnancies. Antunes et al (2019) reported a similar case with anteroposterior deposition of the cervix in a patient, who presented with secondary infertility, after having emergency cesarean section for prolonged labor in her first pregnancy [15]. Mehta et al (2023) documented a case closely paralleling ours, with a history of dyspareunia and difficulty with tampon insertion. The MDA was discovered at the time of Mirena coil insertion. She underwent MRI and subsequent hysteroscopy and resection of septum, like our case, reinforcing the idea that segmental fusion failure—rather than a systemic embryological defect—may underlie these anomalies [13]. However, larger studies and embryologic investigations are necessary to substantiate these evolving hypotheses.
It is known that patients with the more common MDAs (unicornuate, bicornuate, or didelphys) can labor and dilate to have a vaginal delivery. However, by having two cervices and only one cavity, does this impact a patient’s ability to labor? Will the cervices dilate sufficiently? Will one cervix take preference and dilate on its own? From a clinical perspective, the reproductive outcomes in such patients appear largely unaffected, although labor management remains an area of uncertainty. While some reports document successful vaginal deliveries, others note failed labor progress necessitating cesarean sections, with one case opting for a planned elective cesarean section [12–15]. This variability underscores the need for individualized labor planning and further longitudinal studies evaluating cervical dynamics during pregnancy and labor in patients with cervical duplication. With this knowledge, we should be able to inform and counsel patients that they can labor and have a vaginal delivery, however this would have to be on the proviso that there are no other contraindications to vaginal delivery.
This case highlights the importance of careful embryologic interpretation in atypical distal MDAs. From a clinical perspective, failure to recognize such atypical anomalies can lead to misdiagnosis, suboptimal surgical planning, and inadequate reproductive counselling. Accurate classification is essential for informing prognosis, guiding appropriate interventions (e.g., septoplasty vs. metroplasty), and providing patients with realistic expectations regarding fertility, obstetric risk, and mode of delivery. Continued refinement and validation of embryologically grounded classification systems may enhance consistency and developmental clarity in the reporting of rare MDAs.
A critical limitation of our discussion and similar case-based analyses is the lack of embryologic imaging or genetic studies to further explore causation. One of the other limitations in our case report is that our patient has never tried to conceive, so we are unable to determine obstetric outcomes in our case, as with the other case reports. Future research could benefit from combining 3D imaging, fetal MRIs, and molecular embryology to better elucidate the mechanisms responsible for such anomalies. Additionally, further inclusion of recent reviews or systematic analyses (e.g., Santana Gonzalez et al, 2021) on MDA pathogenesis could add depth to the discussion [2].
Conclusions
This case presents a rare variant of Mullerian duct anomaly—duplicated cervices with a single, normally formed uterine cavity and a longitudinal vaginal septum—that challenges long-standing embryologic theories. By highlighting a presentation incompatible with the traditional caudal-to-cranial fusion model, this report adds support to emerging hypotheses suggesting bidirectional or segmental fusion hypothesis, offering a plausible mechanistic explanation for isolated cervical duplication with preservation of a unified uterine corpus. Furthermore, application of the ECC situates this anomaly within Group 3B.2 (cervicovaginal fusion and/or resorption defects), providing precise embryologic localization at the level of the Mullerian tubercle. Unlike many case reports that simply describe anomalies, our analysis contextualizes the findings within both classical and alternative developmental frameworks, reinforcing the need to reconsider how these anomalies are classified and understood.
ASRM and ESHRE classifications remain practical and accessible tools that are easier to interpret and apply in everyday clinical settings. However, embryologically grounded systems, such as the ECC, offer greater developmental specificity and conciseness in describing variant forms of Mullerian duct anomalies. Used together, these systems provide complementary value—combining clinical usability with developmental precision.
Our review of the limited published cases suggests that reproductive outcomes are generally reassuring, with successful conception and vaginal delivery reported in several instances. Although obstetric data remain sparse, current evidence indicates no consistent adverse impact on fertility or on the ability to achieve a healthy pregnancy, provided no additional contraindications are present.
Overall, this case supports a more integrated and developmentally informed approach to classification and counseling in rare cervicovaginal anomalies, while emphasizing the need for continued embryologic and longitudinal clinical research to further refine diagnostic and theoretical models.
Acknowledgments
We would like to thank the patient for consenting to have her case discussed in this report.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
Written consent has been obtained from the patient for publication of this case report and related images.
Author Contributions
LN and MF were involved in the management of this case, reviewing evidence and writing up this report. BH was involved in reviewing the radiographic images and amendments to the paper.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
MDAs: Mullerian duct abnormalities; ASRM: American Society for Reproductive Medicine; ESHRE: European Society of Human Reproduction and Embryology; 3D: three-dimensional; MRI: magnetic resonance imaging; ECC: Embryological–Clinical Classification
| References | ▴Top |
- Chan YY, Jayaprakasan K, Zamora J, Thornton JG, Raine-Fenning N, Coomarasamy A. The prevalence of congenital uterine anomalies in unselected and high-risk populations: a systematic review. Hum Reprod Update. 2011;17(6):761-771.
doi pubmed - Santana Gonzalez L, Artibani M, Ahmed AA. Studying Mullerian duct anomalies - from cataloguing phenotypes to discovering causation. Dis Model Mech. 2021;14(6).
doi pubmed - Acien P, Acien M, Sanchez-Ferrer ML. Mullerian anomalies "without a classification": from the didelphys-unicollis uterus to the bicervical uterus with or without septate vagina. Fertil Steril. 2009;91(6):2369-2375.
doi pubmed - Hashimoto R. Development of the human Mullerian duct in the sexually undifferentiated stage. Anat Rec A Discov Mol Cell Evol Biol. 2003;272(2):514-519.
doi pubmed - Dixit R, Duggireddy CS, Pradhan GS. Mullerian anomalies: revisiting imaging and classification. Insights Imaging. 2025;16(1):40.
doi pubmed - Belle M, Godefroy D, Couly G, Malone SA, Collier F, Giacobini P, Chedotal A. Tridimensional visualization and analysis of early human development. Cell. 2017;169(1):161-173.e112.
doi pubmed - Pfeifer SM, Attaran M, Goldstein J, Lindheim SR, Petrozza JC, Rackow BW, Siegelman E, et al. ASRM mullerian anomalies classification 2021. Fertil Steril. 2021;116(5):1238-1252.
doi pubmed - Grimbizis GF, Gordts S, Di Spiezio Sardo A, Brucker S, De Angelis C, Gergolet M, Li TC, et al. The ESHRE/ESGE consensus on the classification of female genital tract congenital anomalies. Hum Reprod. 2013;28(8):2032-2044.
doi pubmed - Crosby WM, Hill EC. Embryology of the Mullerian duct system. Review of present-day theory. Obstet Gynecol. 1962;20:507-515.
pubmed - Acien P, Navarro V, Acien M. Embryological-clinical classification of female genital tract malformations - a review and update. Reprod Biomed Online. 2025;51(1):104751.
doi pubmed - Muller P, Musset R, Netter A, Solal R, Vinourd JC, Gillet JY. [State of the upper urinary tract in patients with uterine malformations. Study of 133 cases]. Presse Med (1893). 1967;75(26):1331-1336.
pubmed - Deo N, Annan HG. A unique mullerian anomaly of bicollis uterus and vaginal septum with abnormal cervical smears - a case report of pregnancy in such an anomaly. Gynecological Surgery. 2008;5(4):291-292.
- Mehta KM, Wilson EE. A woman with a normal uterus and duplicated cervices: A case report and review of a Mullerian anomaly. Case Rep Womens Health. 2023;37:e00490.
doi pubmed - Morales-Rosello J, Peralta Llorens N. Bicervical normal uterus with normal vagina and anteroposterior disposition of the double cervix. Case Rep Med. 2011;2011:303828.
doi pubmed - Lobo Antunes I, Tomas C, Bravo I, Metello JL, Quintas A, Sa EMP. Double cervix with normal uterus and vagina - an unclassified mullerian anomaly. Int J Fertil Steril. 2019;13(1):83-85.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Clinical Gynecology and Obstetrics is published by Elmer Press Inc.