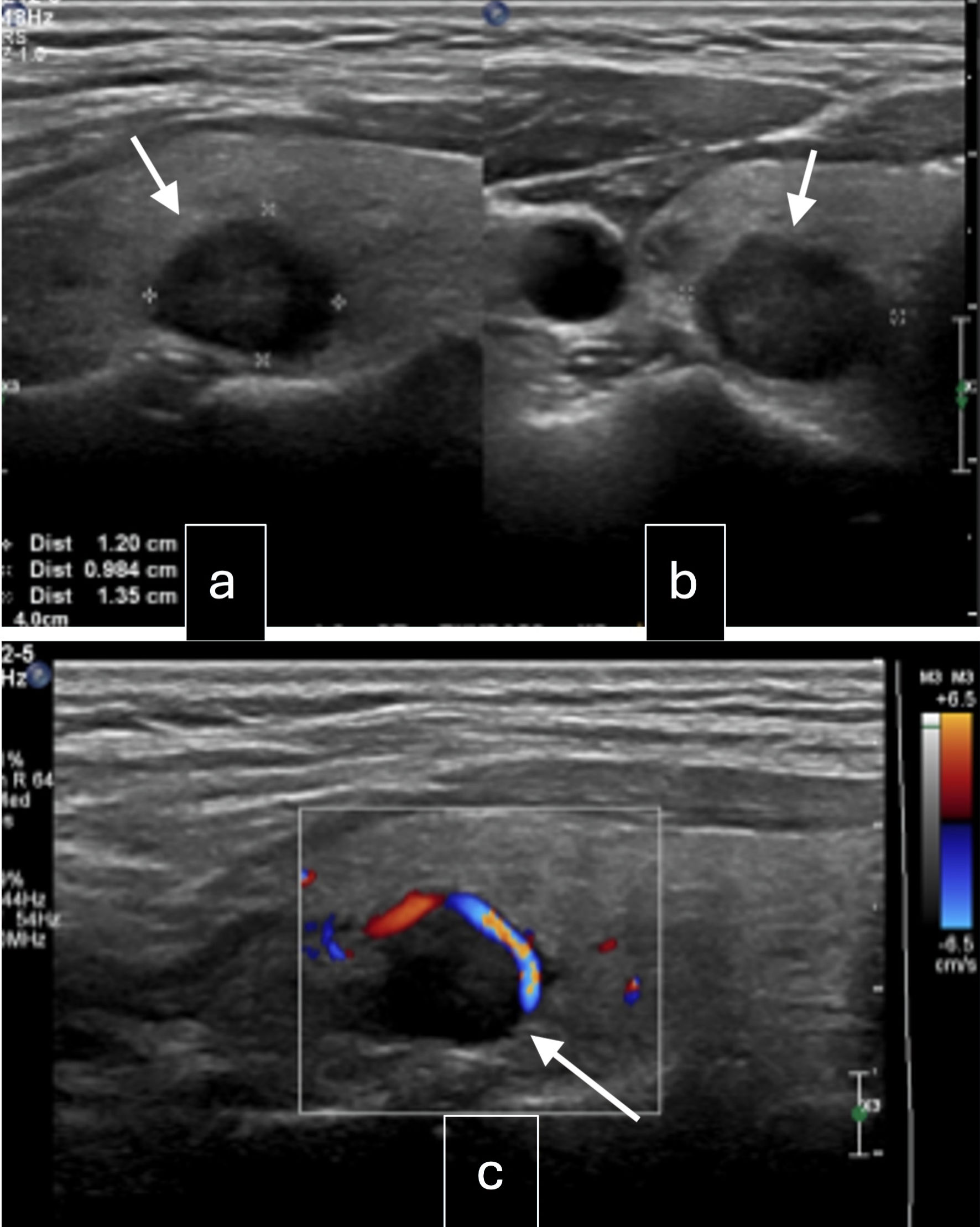
↓ Figure 1. Ultrasound of the neck. (a) Right
lobe mid pole nodule: well-circumscribed, solid, iso-hypoechoic, wider than tall with peripheral
vascularity, 14 × 12 × 10 mm (arrow, intermediate suspicion). (b) Right lobe upper pole
nodule: spongiform lesion, 6 × 4 × 3 mm (arrow, low suspicion). (c) Left lobe mid pole nodule:
well-defined, solid, hypoechoic lesion with coarse internal calcifications, 7 × 7 × 5 mm
(arrow, intermediate suspicion).
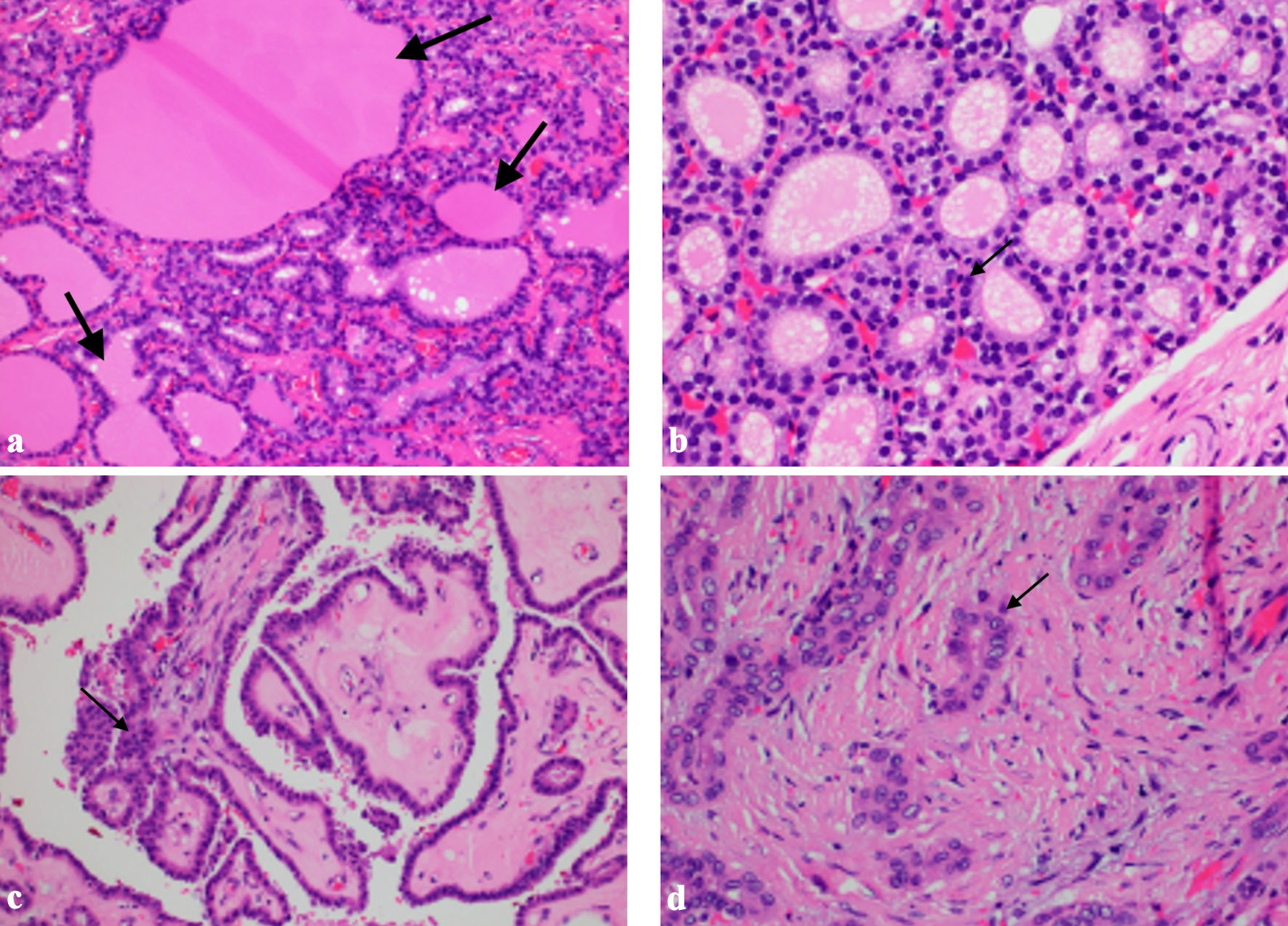
↓ Figure 2. Histology images. (a) Struma ovarii
tissue with evidence of thyroid follicular tissue with colloid seen within the follicles (arrows,
hematoxylin and eosin (HE) × 20). (b) Struma ovarii tissue showing dense nuclei with no nuclear
atypia (arrow, HE × 40). (c) Papillary thyroid carcinoma showing classical papillary formations,
crowded overlapping nuclei (arrow, HE × 20). (d) Papillary thyroid carcinoma showing nuclear
grooves, pseudoinclusions and central clearing (arrow)
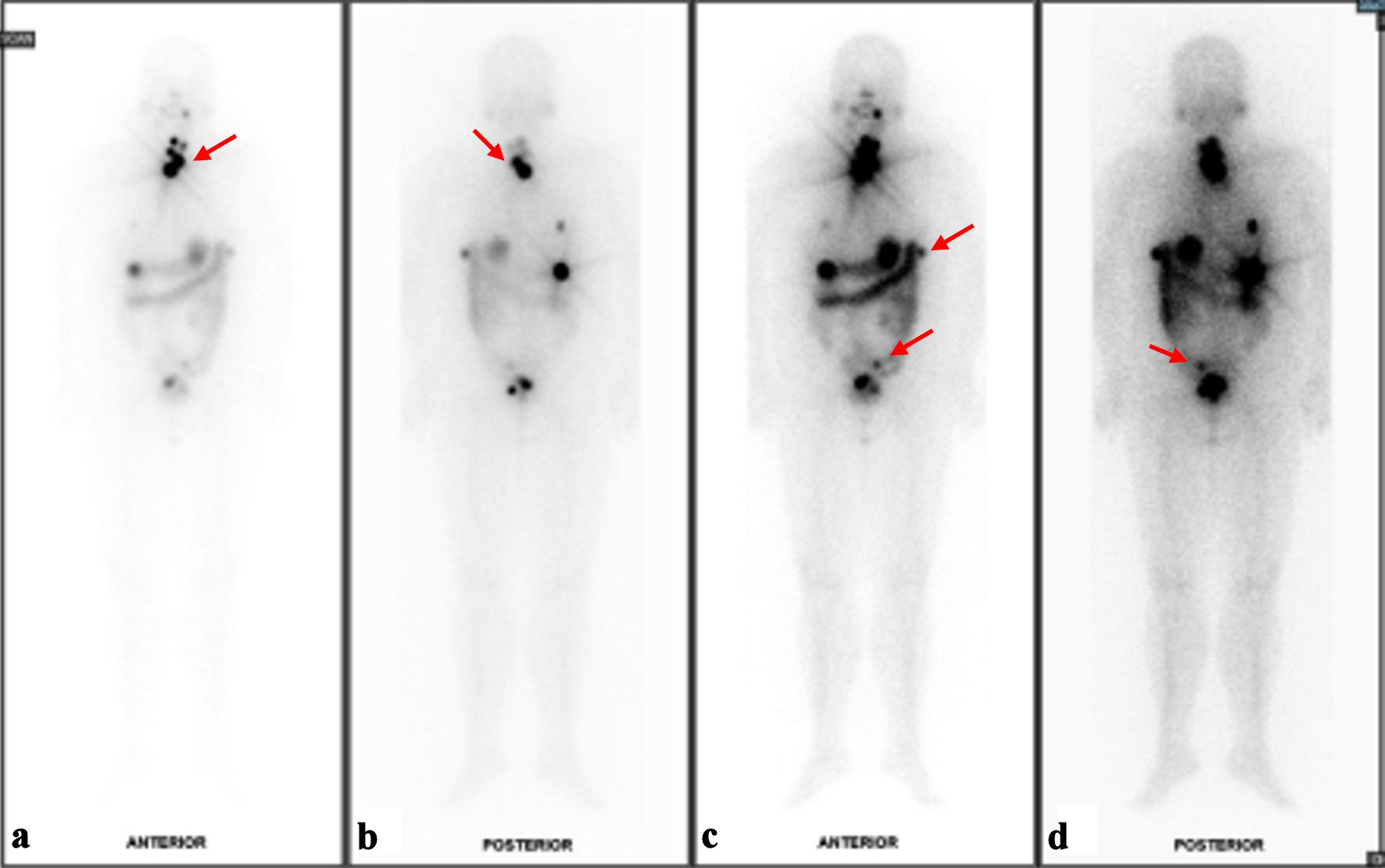
↓ Figure 3. Results of I131 whole body
scan (WBS). (a) Foci of I131 uptake at the anterior neck likely represent remnant thyroid
tissues although small volume disease cannot be ruled out on current baseline study (red arrow). (b)
Posterior view of likely remnant thyroid tissues versus small volume disease (red arrow). (c) Several
I131-avid foci in the upper abdomen and pelvic cavity with corresponding peritoneal
nodules/nodularities are suspicious for residual disease (red arrows). (d) Indeterminate
I131-avid focus at the sigmoid colon region (red arrow).