| Journal of Clinical Gynecology and Obstetrics, ISSN 1927-1271 print, 1927-128X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Gynecol Obstet and Elmer Press Inc |
| Journal website https://jcgo.elmerpub.com |
Original Article
Volume 15, Number 2, June 2026, pages 55-61

Incidence and Maternal Outcomes After Emergency Department Hysterotomy in the Setting of Trauma
Elizabeth Blake Bogina, g ![]() , Michael D. Aprilb, Jonathan S. Hirshbergc, Steven G. Schauerb, d, f, Julie A. Rizzoe, f
, Michael D. Aprilb, Jonathan S. Hirshbergc, Steven G. Schauerb, d, f, Julie A. Rizzoe, f
aThe George Washington University School of Medicine & Health Sciences, Washington, DC, USA
bDepartment of Emergency Medicine, Brooke Army Medical Center, JBSA Fort Sam Houston, TX, USA
cDepartment of Obstetrics and Gynecology, University of Colorado School of Medicine, Aurora, CO, USA
dUS Army Institute of Surgical Research, JBSA Fort Sam Houston, TX, USA
eDepartment of Surgery, Brooke Army Medical Center, JBSA Fort Sam Houston, TX, USA
fThese authors contributed equally as senior authors.
gCorresponding Author: Elizabeth Blake Bogin, The George Washington University School of Medicine, Washington, DC 20037, USA
Manuscript submitted December 9, 2025, accepted January 30, 2026, published online June 6, 2026
Short title: Emergency Department Hysterotomy
doi: https://doi.org/10.14740/jcgo1612
| Abstract | ▴Top |
Background: Trauma in the pregnant patient remains a challenge due the anatomic and physiologic changes that occur. In the setting of extremis, including cardiac arrest, a resuscitative hysterotomy (RH) may be performed to save the life of the mother and often the fetus. The incidence and maternal outcomes of RH in the setting of trauma remain poorly described.
Methods: We analyzed data from the Trauma Quality Improvement Program (TQIP) data registry for any encounter that had documented female sex, diagnosis of pregnancy, and a procedure that involved removal of fetal contents from the uterus in the emergency department (ED).
Results: From 2017 to 2023, there were a total of 8,014,737 total encounters, of which 142 RH procedures occurred in the ED and met inclusion for this analysis. The median maternal age was 27 years (interquartile range (IQR) 22–31, range 16–44). There were 86 (61%) that went straight from the ED to the operating room. The majority received at least one unit of blood products in the first 4 h. The median time from arrival to procedure start was 25 min (IQR 12–50) with the fastest being immediately upon arrival. There were 125 (88%) that had signs of life on arrival. For other resuscitation procedures, there were 48 (34%) that were intubated, one that had a resuscitative endovascular balloon placed, 25 (18%) that received cardiopulmonary resuscitation (CPR), and six (4%) that received a resuscitative thoracotomy. Among those with documented prehospital cardiac arrest, two (10%) survived to hospital discharge. Among those with documented ED CPR, one (4%) survived to hospital discharge. Among those with no signs of life on arrival, none survived to hospital discharge.
Conclusions: RH was exceedingly rare and was associated with a high risk of maternal mortality.
Keywords: Resuscitation; Hysterotomy; Cesarean; Section; Trauma; Obstetric
| Introduction | ▴Top |
Pregnancy influences many physiologic changes to accommodate fetal metabolism, which present a unique set of challenges in the event of a traumatic injury to a pregnant patient [1]. Traumatic injuries are a leading cause of maternal cardiac arrest (MCA), a complex event further complicated by the dual management of the mother and the fetus [2–4]. Cardiac arrest can quickly result in hypoxic brain injury, which occurs faster in a pregnant woman due to alterations in blood composition during pregnancy and increased oxygen demand [5–7]. However, due to the altered fetal hemoglobin configuration, fetuses are relatively resilient to maternal hypoxia [7].
The gravid uterus presents another challenge in managing MCA, because it may impede the provider’s ability to effectively provide chest compressions [6, 8]. Manually generated cardiac output (CO) from compressions is only about 30% of normal CO [8]. Also, after the 20th week of pregnancy, the gravid uterus causes aorto-caval compression and further impedes both venous return and manually generated CO to no more than 10% [6, 8]. Evacuating the uterus rapidly resolves these impediments, and leads to uterine involution, allowing for a large autotransfusion and immediate increase in CO, which has been shown to increase rates of survival following traumatic MCA [5–11].
Resuscitative hysterotomy (RH), previously termed perimortem cesarean section, is critical to caring for the MCA patient. RH is an emergency cesarean section performed on a patient in middle-to-late pregnancy experiencing cardiac arrest, intended to improve the chances of maternal return of spontaneous circulation (ROSC) by reducing the aorto-caval compression caused by the fetus [5–10]. An algorithm for treating MCA is available from the American Heart Association, which suggests that RH should be initiated within 4 min of resuscitative efforts where cardiopulmonary resuscitation (CPR) is initiated but ROSC is not achieved, to facilitate delivery within 5 min [5–8, 12, 13]. In the setting of traumatic MCA, a vertical abdominal incision is recommended for greater visualization, though successful procedures have been documented using a Pfannenstiel incision [5–7]. Some studies suggest that RH can be done to prevent impending cardiovascular collapse, as a peri-arrest intervention, which accounts for longer times between patient arrival and initiation of the RH procedure [7, 9].
While RH is primarily indicated to optimize maternal outcomes, reported maternal and fetal survival rates after RH vary between studies. This is due to a multitude of factors including but not limited to location of arrest (in- or out-of-hospital), time between arrest and RH initiation, and cause of arrest. Studies reported generally high fetal survival rates for neonates > 24 weeks gestation, highlighting the importance of this procedure to fetal outcomes [10]. In RH secondary to traumatic MCA, the available data suggest that it is indicated in accordance with the 4-to-5-min rule, or if maternal survival is impossible [14]. In a study examining four RH patients presenting with hemodynamic instability from traumatic injuries, maternal survival was 50% and fetal survival was reported to be 100% [9]. Conversely, in out-of-hospital MCA, maternal survival is less than half of the national cardiac arrest survival rate (4.5% compared to 9.1%, respectively), and neonatal survival is 10-fold that of their mothers (45%) [10]. Despite these results, similar systematic reviews report higher maternal survival rates, where 54.3% [13] and 54% [6] of MCA patients survived to discharge. Einav et al additionally reported a clear benefit of RH in 31.7% of MCA patients [13].
This heterogeneity of results demands more focused studies of the outcomes of MCA patients undergoing RH to provide clarity and allow for better insight into treatment decisions that will provide the best patient outcomes. Data on the incidence and maternal outcomes in the setting of trauma are lacking, with fetal outcomes oftentimes unavailable. This is a notable limitation in the context of interpreting overall outcomes. Therefore, we sought to determine the maternal outcomes following RH in pregnant females arriving to the emergency department (ED) with traumatic injuries and herein present a descriptive analysis of the latter.
| Materials and Methods | ▴Top |
Ethical statements
We obtained data from the American College of Surgeons Trauma Quality Improvement Program (TQIP) database [4, 15, 16]. The US Army Institute of Surgical Research regulatory office reviewed protocol H-26-003nh and determined that it met the definition of research not involving human subjects. We obtained only de-identified data.
TQIP description
The TQIP database has been maintained by the American College of Surgeons since 2008. The database includes mandatory data collection for level 1 trauma centers and collects data from other centers that do not meet level 1 criteria. The goal of the program is to provide data to aid trauma centers in standardizing trauma care, providing local and national quality improvement, and to provide data needed for best practices guidelines. As of 2023, there are over 800 participating centers where trained registrars enter data for trauma visits that meet entry criteria. The 2023 dataset represents the most recently available dataset as of the time of this analysis.
Case selection
We included cases for which the sex was documented as female and there was a relevant procedure code with a procedure start time that was less than or equal to the ED length of stay (Fig. 1). We assumed that all deliveries performed in the ED were unplanned and emergent. We used the International Classification of Diseases version 10 codes that included any procedure code that starts with the following: 10A, 10D, 10E, 10H, 10J, 10P, 10S, 10T, and 10Y. In addition to the documented procedure, there had to be documentation of a pregnancy diagnostic code and/or the pregnancy preexisting condition variable (available in TQIP 2020-2023; Fig. 1). Other procedures were identified using relevant procedure codes which have been previously described [17, 18]. Due to the use of de-identified data, we could not reliably match maternal data to neonatal data and could not assess neonatal outcomes in conjunction with their corresponding maternal outcomes. As such, we have compiled a description of maternal outcomes noting the limitation of missing neonatal outcomes. Future studies may seek to obtain matched cohorts of maternal and neonatal data for improved insight into how maternal and neonatal outcomes influence one another. Signs of life were defined as a heart rate, respiratory rate, or systolic pressure greater than 0 or a Glasgow coma scale of greater than 3.
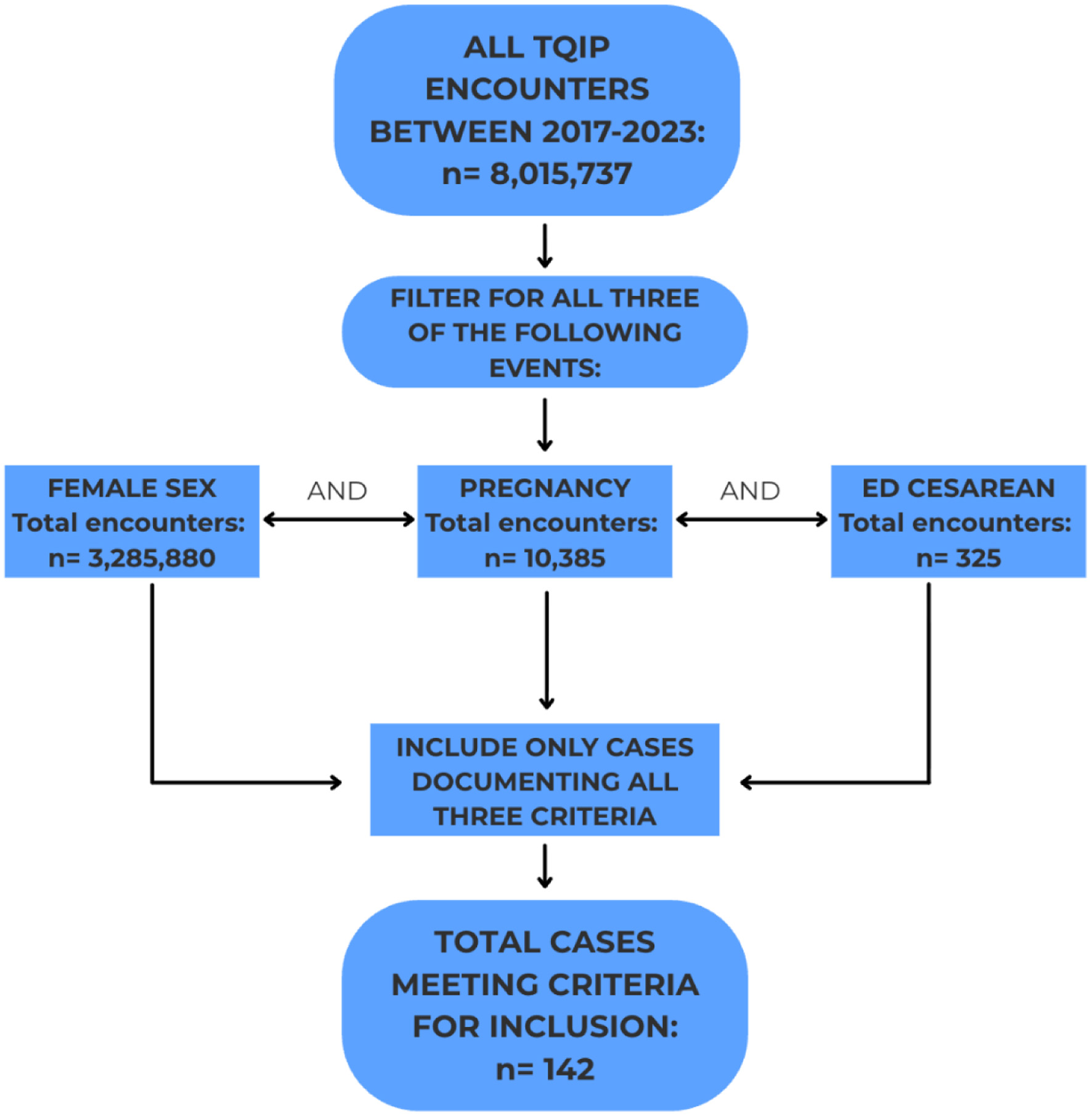 Click for large image | Figure 1. Flow diagram outlining cohort selection. |
Data analysis
We performed all statistical analysis using Microsoft Excel (version 365, Redmond, Washington) and JMP Statistical Discovery from SAS (version 17, Cary, NC). Continuous and ordinal variables are presented with medians and interquartile ranges (IQR). Categorical variables are presented as percentages and numbers.
| Results | ▴Top |
From 2017 to 2023, there were 8,014,737 encounters within the registry datasets. With the datasets, there were 1,850 pregnant patients that had a documented hysterotomy procedure, of which, 142 hysterotomy procedures with a documented pregnancy status occurred in the ED and met inclusion for this analysis (Table 1). Notably, most included cases survived to hospital discharge (Table 1). Pregnancy cases did not document gestational age except in four cases. CPR was not a documented intervention in 100% of the cases included in this analysis, indicating that the 142 cases represent a mixture of RH and peri-arrest cesarean procedures supporting further studies into the indications and outcomes of both procedures. The median maternal age was 27 years (IQR 22–31, range 16–44), and collisions represented the most common mechanism of injury (77%). There were 86 (61%) cases that went straight from the ED to the operating room (OR). The majority received at least one unit of blood products (Fig. 1). The median time from arrival to procedure start was 25 min (IQR 12–50) with the fastest being immediately upon arrival. There were 125 (88%) cases that had signs of life on arrival. For other resuscitation procedures, there were 48 (34%) cases that were intubated, one (< 1%) that had a resuscitative endovascular balloon occlusion of the aorta (REBOA) placed, 25 (18%) that received CPR, and six (4%) that received a resuscitative thoracotomy. Among the 20 cases with documented prehospital cardiac arrest, two (10%) survived to hospital discharge. Among the 25 cases with documented ED CPR, one (4%) survived to hospital discharge. Among those in the study undergoing RH who had no signs of life on arrival (n = 17), none survived to hospital discharge. Of those, 11 were injured in collisions and six were injured by a firearm, representing the two most common mechanisms of injury (Table 1). Of the 142 included cases, there was one that was first trimester, one that was second trimester, and two that were third trimester; the remainder had pregnancy diagnoses that did not specify gestational age. There were six cases that had a concomitant RH and resuscitative thoracotomy, all of which arrived by emergency medical services (EMS) with half experiencing prehospital arrest (Table 2).
 Click to view | Table 1. Patient Characteristics |
Click to view | Table 2. Specific Outcomes of Six Cases Receiving Concomitant Resuscitative Hysterotomy and Resuscitative Thoracotomy |
| Discussion | ▴Top |
The aim of this study was to examine the incidence of RH in the ED following maternal traumatic injury and compare the maternal outcomes to those presented in other studies. Of the 142 cases meeting criteria for inclusion, most patients survived to hospital discharge. Neonatal survival rate is unknown as the dataset is de-identified including dates, times, and locations limiting the ability to link the maternal encounter to the neonatal encounter within the registry. The high survival to discharge is likely reflective of the substantial number that did not have documented arrest upon arrival nor CPR in the ED, suggesting that many of these may have been peri-arrest rather than during an arrest event. As peri-arrest is not a documented scenario, we are suggesting this as an inference that cannot be directly supported by the available data. Moreover, the delayed time from arrival to performance of the procedure in many cases suggests that additional consultative experts may have been available at the bedside that are more experienced in the procedure than emergency physicians (e.g. obstetricians). To that end, the delayed time also allows for more personnel resources to be allocated so the proceduralist could focus on the procedure rather than the totality of the resuscitation.
Small numbers of documented pre-hospital cardiac arrest and ED CPR suggest that RH was primarily performed in a peri-arrest setting, potentially to avoid cardiac arrest in a decompensating patient, and/or to avoid fetal exposure to hemodynamic instability when viability was retained, probably later than 24 weeks gestation. Aftab et al reported similar data in a smaller cohort (n = 4) with available gestational age data, wherein RH was performed in a peri-arrest setting in 75% of patients, and maternal survival rate was 75%, consistent with data reported here [9]. This suggests that not only can RH be used in the setting of maternal cardiac arrest, but it could also be considered as a preventative intervention in a pregnant patient with impending cardiovascular collapse and may improve survival rates if initiated prior to cardiac arrest.
In the 142 cases examined, the median time between patient arrival and initiation of RH was 25 min, similar to results reported by other studies [10]. It is important to note that, while initiation of RH is recommended within 4–5 min of MCA if ROSC is not obtained, when RH is performed in a peri-arrest scenario, time between patient arrival and initiation of RH far exceeds these recommendations [7]. The extended times presented in our dataset, along with the lack of documentation of the time between cardiac arrest and initiation of RH, suggest that many of the procedures may have been performed in a peri-arrest setting, supporting the findings by Aftab et al of increased survival rates in peri-arrest RH patients [9]. However, the lack of documented time between cardiac arrest and RH initiation in many cases is a limitation within the registry as adverse events (e.g. cardiac arrest) are only binary variables and not timed variables. Moreover, the prehospital arrest variable does not include timing factors such as time from arrest to arrival, nor interventions performed by EMS—all factors that can influence outcomes. Another study reported that surviving RH patients had lower recorded times between cardiac arrest and initiation of RH compared to non-surviving patients, supporting the assertion that decreasing the time between arrest and initiation of RH can improve survival rates [7]. While survival is multifactorial and cannot be exclusively attributed to rapid initiation of RH, time is a factor that can increase the odds of survival in viable patients.
The vast majority of traumatic injuries were due to collisions, consistent with other studies assessing RH in the setting of traumatic MCA or maternal injury (Table 1) [1, 9, 10, 14]. Collisions causing traumatic injuries have additional considerations when pregnant patients are involved, due to the physiological changes and increased blood volume, and the injuries could result in RH following MCA or with impending cardiovascular collapse to prevent MCA [1]. Of the 17 patients showing no signs of life on arrival, 11 (65%) were injured in collisions. Though more severe injuries can be mitigated by proper safety precautions such as the use of a seatbelt, they cannot be prevented in the instance of a collision and often necessitate additional interventions to increase maternal survival [1].
Multiple interventions were employed to increase maternal survival, including transfusion of blood products (Fig. 2). About half of patients received at least one unit of blood products with many receiving large volume transfusions, consistent with postoperative resuscitative challenges (Fig. 2) [19]. In addition to transfusion, RH is also useful for relieving aortocaval compression by the gravid uterus in the maternal system and increasing chances of ROSC [6, 8]. Nearly one-third of patients were intubated as part of the resuscitative efforts, which is a procedure that has been noted to have increased difficulty in pregnant women, and often requires an experienced provider [7, 14]. Due to lack of availability of gestational age data, our interpretations of airway management are limited. Six patients underwent concomitant RH and resuscitative thoracotomy, with half showing signs of life on arrival but none surviving to discharge (Table 2). Four (67%) patients who received concomitant RH and resuscitative thoracotomy were injured in collisions (Table 2). Of those, three received blood products, and all received over 4 units of blood products, indicating that severe collision injuries can result in patients in extremis (Table 2; Fig. 2). These cases represent the true extreme of trauma resuscitation procedures with multiple body cavities being opened in the ED. One instance of REBOA was recorded in the cases examined, consistent with attempts to control hemorrhage. The registry does not capture procedure success nor procedure location, so the zone of REBOA placement remains unknown (e.g., high aortic placement versus low pelvic placement).
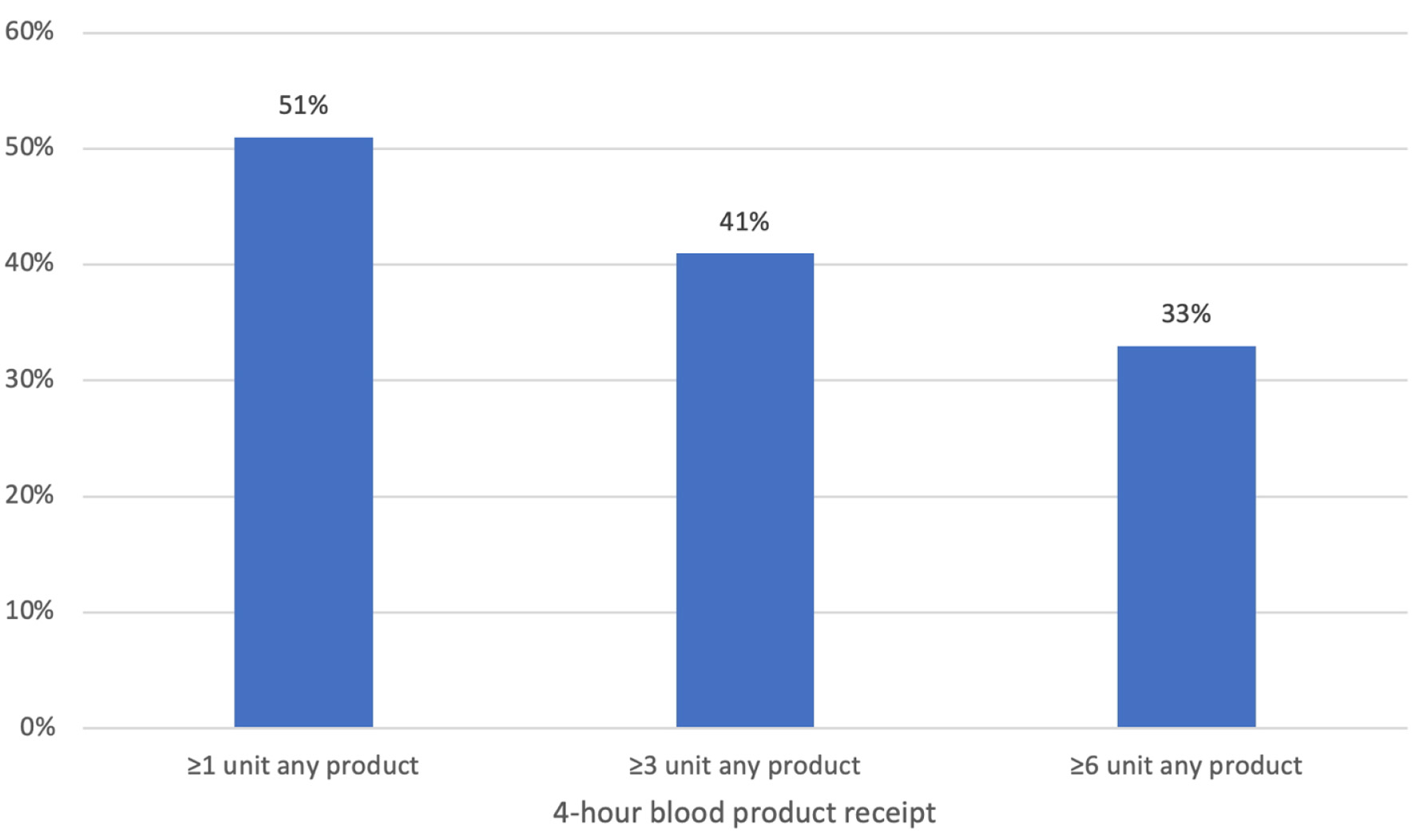 Click for large image | Figure 2. Total 4-h blood products. |
Limitations of this study relate to the extent of available data regarding gestational age and time of cardiac arrest. Only four encounters out of 142 specified a gestational age, which introduces a potential information bias in interpreting maternal survival. Accordingly, results were not interpreted in this context to minimize bias. Another component that was largely absent from the analyzed data were the recorded times between cardiac arrest and initiation of RH. As previously suggested, this may indicate that many patients did not arrest prior to RH or it just was not documented. Future studies may pursue investigating the efficacy of RH as a peri-arrest intervention to prevent complete cardiovascular collapse and increase maternal survival. In conjunction with the limitations mentioned here, other studies found similar limitations in data quality and extent of available data, indicating that more rigorous documentation is needed to continually assess and advance existing knowledge on RH. However, given the exceedingly low frequency of this procedure out of more than 8 million total encounters, large, robust datasets with such details will likely never exist.
Conversely, this study presents a large cohort of RH cases and outcomes, both in the setting of MCA and peri-arrest settings. These cases represent a large sample from many different trauma centers, with data from TQIP, a widely accepted gold-standard for trauma registry data.
Conclusions
Despite the significant limitations in the context of available data, we conclude that incidence of RH was rare and was associated with a high risk of maternal mortality. Due to the low rates of documented CPR, and high rates of survival to discharge, peri-arrest cesarean may serve as a valuable intervention to increase maternal survival in the setting of maternal trauma.
Acknowledgments
We would like to thank the American College of Surgeons for providing us with the data for this study.
Financial Disclosure
None to declare.
Conflict of Interest
MDA, SGS, and JAR have all received funds from the Department of Defense in the form of grants to their institutions. SGS has received funds from SeaStar Medical in the form of grants to his institution for an unrelated effort. None of the military investigators have received external salary support. We have no other conflicts to report.
Disclaimer
The views expressed herein are those of the authors and do not necessarily reflect the official policy or position of the Defense Health Agency, Brooke Army Medical Center, the Department of Defense, nor any agencies under the US Government.
Informed Consent
This study obtained only de-identified data from a publicly available database from the American College of Surgeons and did not involve any direct human interaction; therefore, informed consent was waived.
Author Contributions
EBB performed the literature search and drafted the manuscript. MDA, JSH, SGS, and JAR provided key subject matter expertise and critical revisions. SGS obtained the data and performed the data analysis. All authors contributed substantially.
Data Availability
This study was derived from publicly available data from the American College of Surgeons. We are not authorized to re-share the data.
Abbreviations
CO: cardiac output; CPR: cardiopulmonary resuscitation; ED: emergency department; EMS: emergency medical services; IQR: interquartile range; MCA: maternal cardiac arrest; REBOA: resuscitative endovascular balloon occlusion of the aorta; RH: resuscitative hysterotomy; ROSC: return of spontaneous circulation; TQIP: Trauma Quality Improvement Program
| References | ▴Top |
- April MD, Long B. Trauma in pregnancy: a narrative review of the current literature. Am J Emerg Med. 2024;81:53-61.
doi pubmed - Kilpatrick SJ. Trauma in pregnancy: an underappreciated cause of maternal death. Am J Obstet Gynecol. 2017;217(5):499-500.
doi pubmed - de Assis V, Shields AD, Johansson A, Shumbusho DI, York BM. Resuscitation of traumatic maternal cardiac arrest: A case report and summary of recommendations from Obstetric Life Support. Trauma Case Rep. 2023;44:100800.
doi pubmed - April MD, Fisher AD, Rizzo JA, Wright FL, Winkle JM, Schauer SG. Early vital sign thresholds associated with 24-hour mortality among trauma patients: a trauma quality improvement program (TQIP) study. Prehosp Disaster Med. 2024;39(2):151-155.
doi pubmed - Kikuchi J, Deering S. Cardiac arrest in pregnancy. Semin Perinatol. 2018;42(1):33-38.
doi pubmed - Larson NJ, Mergoum AM, Dries DJ, Hubbard L, Blondeau B, Rogers FB. Perimortem cesarean section after severe injury: What you need to know. J Trauma Acute Care Surg. 2024;97(5):670-677.
doi pubmed - Jeejeebhoy FM, Zelop CM, Lipman S, Carvalho B, Joglar J, Mhyre JM, Katz VL, et al. Cardiac arrest in pregnancy: a scientific statement from the American Heart Association. Circulation. 2015;132(18):1747-1773.
doi pubmed - Gatti F, Spagnoli M, Zerbi SM, Colombo D, Landriscina M, Kette F. Out-of-hospital perimortem cesarean section as resuscitative hysterotomy in maternal posttraumatic cardiac arrest. Case Rep Emerg Med. 2014;2014:121562.
doi pubmed - Aftab N, Halalmeh DR, Vrana A, Smitterberg C, Cranford JA, Sachwani-Daswani GR. Enhancing maternal survival in traumatic cardiovascular collapse during pregnancy: a case series on resuscitative hysterotomy (RH) from a level 1 trauma center. Injury. 2025;56(1):111923.
doi pubmed - Leech C, Nutbeam T, Chu J, Knight M, Hinshaw K, Appleyard TL, Cowan S, et al. Maternal and neonatal outcomes following resuscitative hysterotomy for out of hospital cardiac arrest: A systematic review. Resuscitation. 2025;207:110479.
doi pubmed - Nagraj S, Kong S. Maternal cardiac arrest: the present and the future. Future Cardiol. 2024;20(3):99-101.
doi pubmed - American Heart Association. Cardiac arrest in pregnancy in-hospital ACLS algorithm. Published online 2020.
- Einav S, Kaufman N, Sela HY. Maternal cardiac arrest and perimortem caesarean delivery: evidence or expert-based? Resuscitation. 2012;83(10):1191-1200.
doi pubmed - Mendez-Figueroa H, Dahlke JD, Vrees RA, Rouse DJ. Trauma in pregnancy: an updated systematic review. Am J Obstet Gynecol. 2013;209(1):1-10.
doi pubmed - Lin LC, April MD, Douin DJ, Winkle JM, Jenson WR, Rizzo JA, Schauer SG. Airway management in trauma patients: A seven-year review of emergency department intubations. Am J Emerg Med. 2026;99:306-312.
doi pubmed - Le DM, Douin DJ, Tanabe KJ, April MD, Schauer SG. Emergency department use of airway adjuncts in the setting of endotracheal intubation for traumatic injury. J Emerg Med. 2025;79:82-90.
doi pubmed - Krepps AR, Douin DJ, Winkle JM, Wright FL, Fisher AD, April MD, Schauer SG. Characterizing emergency department surgical airway placement in the setting of trauma. Am J Emerg Med. 2024;85:48-51.
doi pubmed - Hanif H, Fisher AD, April MD, Rizzo JA, Miskimins R, Dubose JD, Cripps MW, et al. An assessment of nationwide trends in emergency department (ED) resuscitative endovascular balloon occlusion of the aorta (REBOA) use - A trauma quality improvement program registry analysis. Am J Surg. 2024;238:115898.
doi pubmed - Shields AD, Vidosh J, Zelop CM. Resuscitative cesarean delivery: when every second counts. Am J Obstet Gynecol. 2026;233(6S):S272-S279.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Clinical Gynecology and Obstetrics is published by Elmer Press Inc.