| Journal of Clinical Gynecology and Obstetrics, ISSN 1927-1271 print, 1927-128X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Gynecol Obstet and Elmer Press Inc |
| Journal website https://jcgo.elmerpub.com |
Original Article
Volume 14, Number 4, December 2025, pages 176-183

Impact of Severe Male Factor Infertility on In Vitro Fertilization-Intracytoplasmic Sperm Injection Outcomes: A Retrospective Cohort Study
Sholen Acharyaa, c, Sheila Balakrishnana, Reji Mohana, Deepak Rathb
aDepartment of Reproductive Medicine and Surgery, Government Medical College,
Thiruvananthapuram, India
bDepartment of Internal Medicine, John H. Stroger, Jr.
Hospital of Cook County, Chicago, IL, USA
cCorresponding Author: Sholen Acharya,
Department of Reproductive Medicine and Surgery, Government Medical College, Thiruvananthapuram,
India
Manuscript submitted September 8, 2025, accepted November 26, 2025, published online December 11,
2025
Short title: Impact of Severe Male Factor Infertility on IVF
doi:
https://doi.org/10.14740/jcgo1548
| Abstract | ▴Top |
Background: Severe male factor infertility presents challenges in assisted reproductive technology (ART). This study evaluated whether severe male factor infertility impacts clinical pregnancy outcomes following in vitro fertilization-intracytoplasmic sperm injection (IVF-ICSI) compared to non-male factor cases.
Methods: In this retrospective cohort study at the Department of Reproductive Medicine and Surgery, SAT Hospital, Government Medical College, Thiruvananthapuram, couples undergoing IVF-ICSI between January 2017 and December 2020 were divided into severe male factor (group 1, n = 51) and non-male factor (group 2, n = 51) groups, matched for female age, body mass index, and ovarian reserve. Outcomes compared included clinical pregnancy rates (CPRs) based on sperm source (ejaculated vs. surgically retrieved) and male factor type (severe oligoasthenoteratozoospermia vs. azoospermia). Statistical analysis utilized univariate and multivariate logistic regression.
Results: The overall CPR was 75.5%. Group 1 (severe male factor) achieved a CPR of 68.6%, while group 2 (non-male factor) achieved 82.4%, a difference that was not statistically significant (P = 0.107). Within group 1, no significant differences were found between outcomes using ejaculated versus surgically retrieved sperm (P = 0.393). Logistic regression showed lower odds of pregnancy with severe male factor infertility (odds ratio 0.469, 95% confidence interval: 0.185 - 1.190), but this was not statistically significant (P = 0.111).
Conclusion: Severe male factor infertility, including cases requiring surgical sperm retrieval, does not significantly compromise CPRs in IVF-ICSI cycles when female factors and treatment protocols are optimized.
Keywords: Severe male infertility; IVF-ICSI; Azoospermia; Oligoasthenoteratozoospermia; Surgical sperm retrieval; Clinical pregnancy rate
| Introduction | ▴Top |
Infertility affects one in six people, which is 17.5% of the adult population globally [1], with male factors contributing to nearly half of these cases either alone or in combination with female factors [2]. Severe male factor infertility, encompassing conditions such as severe oligoasthenoteratozoospermia (OAT) and azoospermia, presents unique challenges in assisted reproductive technology (ART) programs. The advent of intracytoplasmic sperm injection (ICSI) has revolutionized the management of severe male infertility by enabling successful fertilization with minimal viable spermatozoa [3]. However, questions persist regarding the impact of compromised sperm quality on embryo development, implantation, and clinical pregnancy rates (CPRs), particularly when compared to in vitro fertilization-intracytoplasmic sperm injection (IVF-ICSI) outcomes in couples without male factor infertility.
Some studies suggest that despite poor semen parameters, ICSI can largely overcome male infertility, resulting in clinical pregnancy and live birth rates comparable to those of non-male factor infertility cases [4]. Conversely, concerns have been raised that sperm from severely affected males may harbor higher rates of DNA fragmentation or epigenetic alterations, potentially influencing reproductive outcomes [5].
This retrospective cohort study aimed to assess whether severe male factor infertility affects clinical pregnancy outcomes following IVF-ICSI in a matched cohort at a tertiary care center. By comparing couples affected by severe male factor infertility to those without, and further evaluating outcomes based on the sperm source (ejaculated vs. surgically retrieved), this study aimed to offer clinically relevant insights into how the severity of male infertility influences outcomes in contemporary ART practice.
| Materials and Methods | ▴Top |
Study design and setting
This retrospective cohort study was conducted at the Department of Reproductive Medicine and Surgery, Sri Avittom Thirunal (SAT) Hospital, Government Medical College, Thiruvananthapuram, Kerala. Ethical clearance was obtained from the Institutional Ethics Committee before initiating the study. Patient records from January 1, 2017, to December 31, 2020, were reviewed to identify eligible couples who had undergone IVF with ICSI.
Participant selection
The study included couples undergoing IVF-ICSI treatment and was categorized into two cohorts: Group 1 (severe male factor group): couples with severe male factor infertility who underwent IVF-ICSI using autologous sperm, either ejaculated or surgically retrieved; group 2 (non-male factor group): couples with no male factor infertility, including a small subset with azoospermia managed via donor sperm.
To reduce bias, female partners in both groups were matched for age, body mass index (BMI), and ovarian reserve markers (anti-Müllerian hormone (AMH), antral follicle count (AFC)), factors known to influence IVF outcomes [6]. Couples were excluded if the female partner had diminished ovarian reserve, or confounding uterine or endometrial pathologies, such as endometriosis, adenomyosis, fibroids, or hydrosalpinx.
Due to limited donor sperm IVF-ICSI cycles at our center, the control group (group 2) primarily comprised women with infertility related to polycystic ovary syndrome (PCOS), tubal block, or unexplained causes, where oocyte quality and endometrial receptivity were not severely compromised. A sample size calculation, based on a presumed 60% CPR in PCOS patients undergoing IVF [7] and an expected 50% reduction due to male factor infertility [8], indicated that 40 couples per group would achieve 95% confidence and 80% power. We recruited 51 couples in each group.
Data collection
Baseline demographic and clinical data were extracted from patient records into Microsoft Excel. All couples had undergone a comprehensive infertility workup including hormonal evaluation (follicle-stimulating hormone (FSH), luteinizing hormone (LH), thyroid-stimulating hormone (TSH), prolactin (PRL)), ovarian reserve assessment (AMH, AFC), transvaginal ultrasound for female partners, and semen analysis for male partners. Semen analysis followed WHO guidelines and was performed after 2 - 3 days of abstinence using ejaculated samples obtained via masturbation.
Severe male factor infertility was defined as: 1) severe OAT: sperm concentration < 16 million/mL, progressive motility < 30%, normal morphology < 4% [9]; 2) azoospermia: complete absence of sperm in the ejaculate.
The source of sperm - ejaculate, surgically retrieved, or donor - was documented, along with IVF outcomes including embryo development and clinical pregnancy, defined as visualization of an intrauterine gestational sac on ultrasound.
IVF-ICSI and embryo transfer procedures
Procedures were performed according to standardized institutional protocols, as previously published [10]. Key steps included the following.
Ovarian stimulation and oocyte retrieval
Controlled ovarian stimulation using gonadotropin-releasing hormone (GnRH) antagonist or long agonist protocols, with human menopausal gonadotropin (HMG) (MENOPUR) or recombinant FSH (GONAL-F), was tailored to individual ovarian reserve. Final oocyte maturation was triggered using human chorionic gonadotropin (hCG), GnRH agonist, or dual trigger, followed by ultrasound-guided oocyte retrieval 35 h later.
Sperm collection and preparation
Ejaculated sperm was processed using a two-layer (40%/80%) discontinuous density gradient centrifugation.
Surgically retrieved sperm was obtained through percutaneous epididymal sperm aspiration (PESA) performed under local anesthesia using a 23-G needle to aspirate epididymal fluid or through testicular sperm aspiration (TESA) performed with an 18-G needle to aspirate testicular tissue for sperm extraction.
ICSI, fertilization, and embryo culture
ICSI was performed on all mature oocytes (metaphase II), using a micromanipulator under an inverted microscope. A single, motile, morphologically normal sperm was immobilized and injected into the oocyte cytoplasm. Fertilization was assessed 16 h post-ICSI. Embryos were cultured in G-TL medium and graded based on the Istanbul consensus.
Cryopreservation and embryo transfer
Embryos were vitrified using the Kitazato Cryotop method as per the center’s “all-freeze” policy. In frozen embryo transfer (FET) cycles, endometrial preparation involved estradiol valerate and progesterone, with or without GnRH agonist downregulation. Embryos were warmed, cultured, and graded for transfer using Istanbul criteria (cleavage/morula) or Gardner and Schoolcraft system (blastocysts). Transfer was performed under transabdominal ultrasound guidance using a Sydney IVF catheter.
Luteal support and pregnancy confirmation
Post-transfer, luteal support was provided with vaginal progesterone gel. Serum β-hCG was measured 12 days after embryo transfer. Clinical pregnancy was confirmed by ultrasound at 6 weeks.
Outcome measures
The primary outcome was clinical pregnancy, defined as the presence of an intrauterine gestational sac, with or without a fetal pole. Pregnancy rates were compared between groups (male factor vs. non-male factor infertility), with further subgroup analyses by type of male factor (severe OAT vs. azoospermia) and sperm source (ejaculate, surgically retrieved, donor).
Statistical analysis
Statistical analysis was performed using Jamovi software [11]. Continuous variables were tested for normality using Shapiro-Wilk test and expressed as mean ± standard deviation (SD) and median. Categorical variables were analyzed using Chi-square test and continuous variables using Student’s t-test (normal distribution) or Mann-Whitney U test (non-normal distribution). A univariate logistic regression model was used to examine the association between male factor infertility (using autologous sperm) and clinical pregnancy outcome. A multivariate logistic regression model was constructed to control for potential confounders including female age, BMI, AMH, and AFC, and to identify independent predictors of IVF-ICSI success. A two-tailed P-value < 0.05 was considered statistically significant.
Ethical considerations
This study was conducted in accordance with the ethical standards of the Institutional Ethics Committee of Government Medical College, Thiruvananthapuram, and with the 1964 Helsinki declaration and its later amendments. Ethical approval was obtained prior to the initiation of the study.
| Results | ▴Top |
Clinical characteristics of study participants
In group 1 (n = 51), male factor infertility was present in all cases, with 66.7% (n = 34) diagnosed with severe OAT and 33.3% (n = 17) with azoospermia. Female factor (PCOS) was present in 21.6% of couples. The source of sperm was ejaculate in 64.7% and surgically retrieved in 35.3% (Table 1).
 Click to view |
Table 1. Distribution of Male Factor, Female
Factor, and Source of Sperm Between Two Study Groups |
In group 2 (n = 51), there was no male factor as those with azoospermia (n = 3, 5.9%) were managed with donor sperms. The causes of infertility included female factor like PCOS (43.1%, n = 22), tubal block (15.7%, n = 8), and unexplained infertility (35.3%, n = 18). There was significant difference between group 1 and group 2 in terms of male and female factor as well as sperm source.
Baseline female partner characteristics
Female age, BMI, AMH, and AFC were comparable between the two groups. Age and BMI were normally distributed and analyzed using Student’s t-tests, while AMH and AFC were non-normally distributed and compared using the Mann-Whitney U test (Table 2).
Click to view |
Table 2. Distribution of Female Age, BMI, and
Ovarian Reserve Markers Between Two Study Groups |
Outcome measures
The overall CPR across both groups was 75.5% (77 out of 102 couples). In group 1, which consisted of couples with severe male factor infertility, the CPR was 68.6% (35/51), while in group 2, which included couples without male factor infertility (including those using donor sperm), the pregnancy rate was 82.4% (42/51); however, this difference did not reach statistical significance (P = 0.107). On comparing outcome between ejaculated sperms with male factor vs. ejaculated sperms without male factor, there was no significant difference in the CPRs (P = 0.365). Similarly, among couples using surgically retrieved sperm in group 1, the pregnancy rate was 64.7% (11/18), which again was not significantly different when compared to the 100% pregnancy rate observed in the small number of donor sperm users in group 2 (3/3 couples, P = 0.219) (Table 3).
Click to view |
Table 3. Clinical Pregnancy Distribution
Between Study Groups |
Within the male factor group (group 1), couples with severe OAT had a CPR of 70.6% (24/34), while those with azoospermia had a slightly lower CPR of 64.7% (11/17), with no significant difference (P = 0.670), indicating similar treatment success regardless of severity of male factor condition. When comparing sperm source within group 1, those using ejaculated sperm had a higher CPR (72.7%, 24/33) compared to those using surgically retrieved sperm (61.1%, 11/18), although this difference too was not statistically significant (P = 0.393), suggesting that both methods of sperm acquisition can yield comparable pregnancy outcomes in the context of IVF-ICSI.
Regression analysis
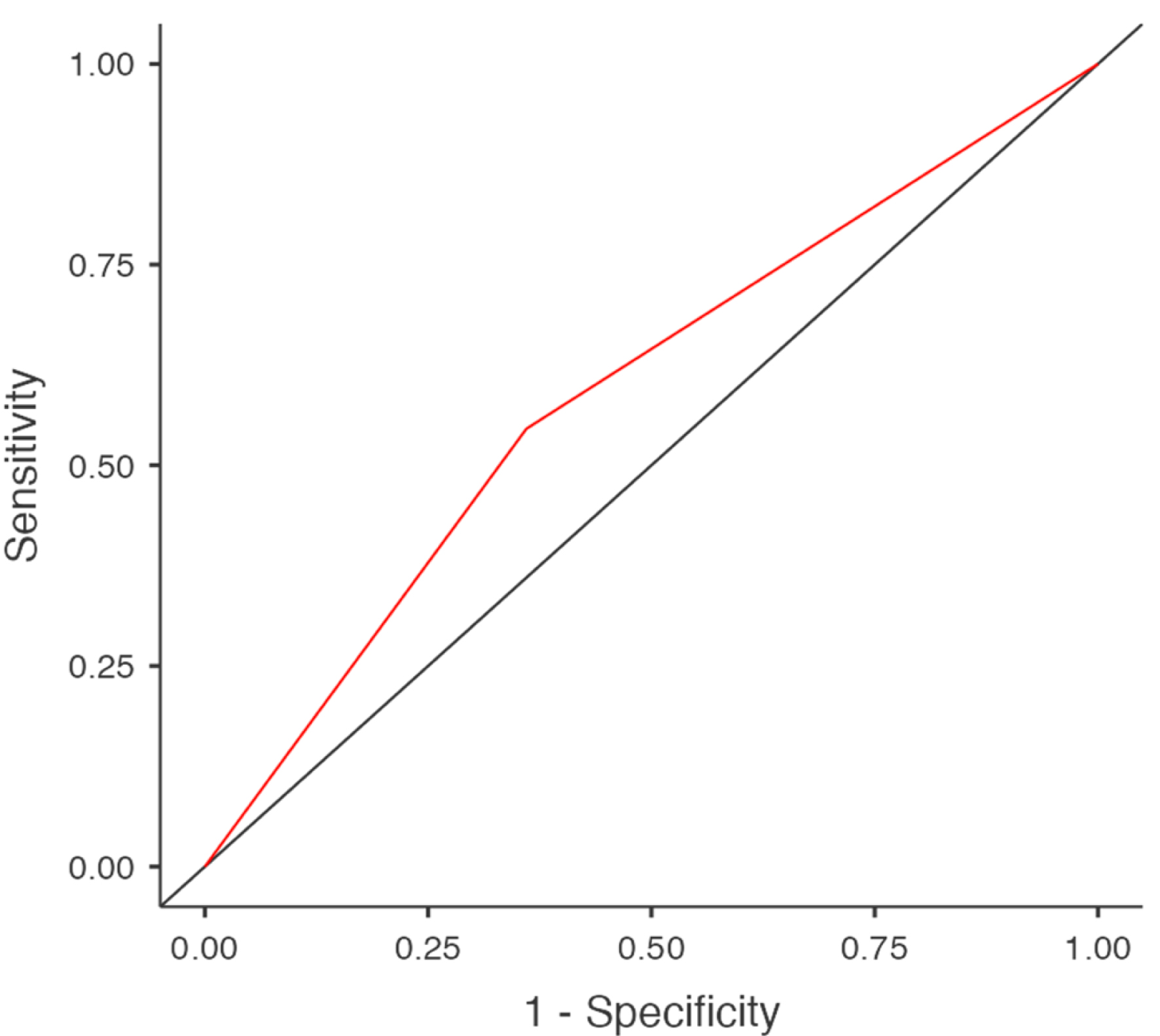
Logistic regression analysis was performed using both groups to evaluate whether the presence of severe male factor infertility impacted IVF-ICSI outcomes. The univariate model (Table 4) showed that male factor infertility was associated with lower odds of achieving pregnancy (odds ratio (OR) 0.469 (95% confidence interval (CI): 0.185 to 1.190)), but this was not statistically significant (P = 0.111). The model explained only a small proportion of variance in outcomes (McFadden’s R2 = 0.0231). The receiver operating characteristic (ROC) analysis of this model (Fig. 1) demonstrated perfect sensitivity (1.00), identifying all pregnancies correctly, but failed to distinguish non-pregnancies (specificity = 0.00), with an area under the curve (AUC) of just 0.593, reflecting poor discriminative ability.
Click to view |
Table 4. Univariate Logistic Regression Model
Assessing the Impact of Severe Male Factor Infertility (Group 1 vs. Group 2) on
Clinical Pregnancy Outcomes Following IVF-ICSI |
 Click for large image |
Figure 1. Receiver operating characteristic (ROC) curve illustrating the predictive performance of severe male factor infertility status on pregnancy outcome in IVF-ICSI cycles. Area under curve (AUC) = 0.593. IVF-ICSI: in vitro fertilization-intracytoplasmic sperm injection. |
To adjust for potential confounders, a multivariate logistic regression analysis (Table 5) was conducted, including age, BMI, AMH, and AFC as covariates. Male factor infertility remained a non-significant predictor of pregnancy (adjusted OR = 0.440, 95% CI: 0.159 to 1.22, P = 0.115), and none of the additional covariates significantly impacted the likelihood of pregnancy either (all P-values > 0.05), reinforcing the notion that neither male factor status nor baseline female characteristics were strong independent predictors of clinical pregnancy in this cohort undergoing IVF-ICSI.
Click to view |
Table 5. Multivariate Logistic Regression Model
Evaluating the Association Between Severe Male Factor Infertility and Clinical
Pregnancy Following IVF-ICSI, Adjusting for Female Partner Characteristics (Age,
BMI, AMH, and AFC) |
| Discussion | ▴Top |
This study aimed to evaluate the impact of severe male factor infertility on IVF-ICSI outcomes by comparing CPRs between couples with severe male factor infertility (group 1) and those without (group 2), with further stratification based on the type of male factor and source of sperm used. Despite numerical differences in pregnancy rates between groups, our findings suggest that severe male factor infertility, including cases requiring surgical sperm retrieval, does not significantly compromise clinical pregnancy outcomes in IVF-ICSI cycles when appropriate techniques and laboratory standards are employed.
Group 1 consisting of couples with either severe OAT or azoospermia using autologous sperm, achieved a CPR of 68.6%, while group 2, comprising couples without male factor infertility (including those who used donor sperm), showed a higher, though statistically non-significant, pregnancy rate of 82.4% (P = 0.107). This finding reinforces the current understanding that ICSI is a highly effective technique for overcoming poor semen parameters, allowing fertilization and pregnancy rates to approach those seen in non-male factor cases. Those with prior fertilization failures have seen improved outcome due to the technique of aggressive sperm immobilization used in ICSI [12].
When comparing outcomes based on sperm source, couples using ejaculated sperm in the presence of male factor infertility achieved a CPR of 72.7%, which was not significantly different from the 81.3% seen in those using ejaculated sperm without male factor (P = 0.365). ICSI has shown higher success rates in male infertility but not improves outcomes in those without male factor compared to conventional IVF, indicating its specific advantage in male infertility [13]. The CPR among couples using surgically retrieved sperm was 64.7%, which also did not differ significantly from the 100% success rate observed in a small number of donor sperm cycles (P = 0.219). Although the use of donor sperm yielded excellent results, the limited number of cases (n = 3) precludes definitive conclusions. Other studies have consistently shown that donor sperms have higher IVF success rates compared to partner sperm in severe male infertility [14, 15]. Due to limited donor IVF cycles at our center, we were unable to draw conclusive results. But our study shows that using partner sperm in severe male infertility with ICSI gives a viable option and has comparable results to those without male factor.
Within the severe male factor group, CPRs did not differ significantly between those with severe OAT (70.6%) and those with azoospermia (64.7%) (P = 0.670). Moreover, when comparing sperm acquisition methods within this group, ejaculated sperm yielded a higher pregnancy rate (72.7%) compared to surgically retrieved sperm (61.1%), though the difference was not statistically significant (P = 0.393). These observations are clinically important, as they support the use of surgical sperm retrieval in azoospermic men without expecting a substantial compromise in treatment outcomes. The success of ICSI is highly dependent on the selection of viable sperm, and techniques like using testicular spermatozoa or aggressive sperm immobilization can further enhance outcomes [12, 16].
Regression analyses further substantiated these observations. The univariate logistic model indicated a trend toward lower odds of pregnancy in cases with severe male factor infertility (OR = 0.469), though the association was not statistically significant (P = 0.111). The multivariate analysis, which controlled for female age, BMI, AMH, and AFC, also failed to identify male factor status or any female partner variables as independent predictors of clinical pregnancy, reinforcing the conclusion that with good female parameters and standardized treatment protocols, male factor infertility does not independently reduce the likelihood of conception.
The rigorous inclusion criteria of this study, excluding couples with diminished ovarian reserve or endometrial factors, allowed for a focused examination of the male factor’s impact, minimizing confounding influences. Furthermore, standardized stimulation, ICSI, culture, and transfer protocols reduced procedural variability, enhancing the internal validity of the findings.
The limitations of this study include its retrospective design and single-center setting, which may limit generalizability. The sample size was relatively small, particularly in the donor sperm subgroup, reducing the power to detect subtle but clinically meaningful differences. Due to limited cases, azoospermia could not be stratified into obstructive and non-obstructive types, and subgroup analyses based on the method of surgical sperm retrieval (PESA vs. TESE) were not feasible. Additionally, although tubal factor alone would have been the optimal comparator, the scarcity of such cases without hydrosalpinx necessitated the inclusion of selected PCOS and unexplained infertility cases in the control group. Furthermore, key outcome measures such as live birth rate, take-home baby rate, embryonic euploidy data, and offspring health metrics were not available. Future well-designed, prospective multicentric studies with larger cohorts, stricter grouping criteria, and key outcome measures such as live birth rate, take-home baby rate, embryonic euploidy data, and offspring health metrics should be done to better assess the ability of IVF/ICSI to overcome male factor infertility.
Conclusion
This study demonstrates that the presence of severe male factor infertility, including azoospermia requiring surgical sperm retrieval, does not significantly impact clinical pregnancy outcomes in IVF-ICSI cycles when female partner characteristics are comparable and standard ART protocols are followed. These results provide reassurance for couples with severe male factor infertility and support the continued use of ICSI with autologous sperm, whether ejaculated or surgically retrieved, as an effective treatment option.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
The authors declare that there is no conflict of interest.
Informed Consent
As this was a retrospective analysis of anonymized patient data, the requirement for individual informed consent was waived by the Institutional Ethics Committee.
Author Contributions
SA was responsible for conceptualization, data curation, and formal analysis, contributed to methodology design, software development, and data visualization, drafted the original manuscript and participated in subsequent review and editing. SB contributed to the conceptualization and methodological framework, was responsible for investigation, project administration, and resource management, provided supervision, supported validation, assisted with visualization, and took part in reviewing and editing the manuscript. RM contributed to conceptualization, was responsible for investigation, project administration, resource management, supervision, and took part in reviewing and editing the manuscript. DR contributed to conceptualization, visualization, took the lead in data curation, formal analysis, and software development, assisted with methodology and validation, and was actively involved in drafting the original manuscript as well as reviewing and editing.
Data Availability
The datasets generated and/or analyzed during the current study are available in the Mendeley data repository [17].
| References | ▴Top |
- 1 in 6 people globally affected by infertility: WHO. Accessed November 23, 2025. https://www.who.int/news/item/04-04-2023-1-in-6-people-globally-affected-by-infertility.
- Agarwal A, Mulgund A, Hamada A, Chyatte MR. A unique view on male
infertility around the globe. Reprod Biol Endocrinol. 2015;13:37.
doi pubmed - Palermo G, Joris H, Devroey P, Van Steirteghem AC. Pregnancies after
intracytoplasmic injection of single spermatozoon into an oocyte. Lancet.
1992;340(8810):17-18.
doi pubmed - Esteves SC, Roque M, Bedoschi G, Haahr T, Humaidan P.
Intracytoplasmic sperm injection for male infertility and consequences for offspring. Nat Rev
Urol. 2018;15(9):535-562.
doi pubmed - Zini A, Sigman M. Are tests of sperm DNA damage clinically useful?
Pros and cons. J Androl. 2009;30(3):219-229.
doi pubmed - Shingshetty L, Cameron NJ, McLernon DJ, Bhattacharya S. Predictors of
success after in vitro fertilization. Fertil Steril. 2024;121(5):742-751.
doi pubmed - Nguyen TH, Nguyen TTD, Le HT, Vo TKQ, Le TTA. Research on clinical
pregnancy rate and some factors related to IVF outcomes in women with polycystic ovary syndrome
at Can Tho Obstetrics and Gynecology Hospital. TC Phu san. 2024;22(2):59-67.
doi - Riffenburgh RH, Gillen DL. Sample size estimation. In: Statistics in
Medicine. Elsevier; 2020:533-563.
doi - Campbell M. Fertile man semen parameters 2020 - an update to the data
collated for the WHO semen analysis manual 2010. Published online 2021:223 KB.
doi - Acharya S, Balakrishnan S, Rath D. Pregnancy rates after frozen
embryo transfer: insights from an Indian Government Hospital. IJMRGE. 2025;6(2):965-972.
doi - The jamovi project (2024). jamovi. (Version 2.6) [Computer Software]. https://www.jamovi.org.
- Chou CW, Chen SU, Chang CH, Tsai YY, Huang CC. Aggressive sperm
immobilization improves reproductive outcomes in patients with suboptimal semen parameters and
previous ICSI fertilization failure. Sci Rep. 2024;14(1):5363.
doi pubmed - Boulet SL, Mehta A, Kissin DM, Warner L, Kawwass JF, Jamieson DJ.
Trends in use of and reproductive outcomes associated with intracytoplasmic sperm injection.
JAMA. 2015;313(3):255-263.
doi pubmed - Mignini Renzini M, Dal Canto M, Guglielmo MC, Garcia D, De Ponti E,
La Marca A, Vassena R, et al. Sperm donation: an alternative to improve post-ICSI live birth
rates in advanced maternal age patients. Hum Reprod. 2021;36(8):2148-2156.
doi pubmed - Cai H, Gordts S, Sun J, Meng B, Shi J. Reproductive outcomes with
donor sperm in couples with severe male-factor infertility after intracytoplasmic sperm
injection failures. J Assist Reprod Genet. 2020;37(8):1883-1893.
doi pubmed - Chen T, Fan D, Wang X, Mao C, Chu Y, Zhang H, Liu W, et al. ICSI
outcomes for infertile men with severe or complete asthenozoospermia. Basic Clin Androl.
2022;32(1):6.
doi pubmed - Acharya S. Dataset for impact of severe male factor infertility on
IVF-ICSI outcomes: a retrospective cohort study. Published online 2025.
doi
This
article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0
International License, which permits unrestricted non-commercial use, distribution, and
reproduction in any medium, provided the original work is properly cited.
Journal
of Clinical Gynecology and Obstetrics is published by Elmer Press Inc.